ECHO Institute, University of New Mexico, Albuquerque, NM, USA.
Department of Statistics, University of New Mexico School of Medicine, Albuquerque, NM, USA.
J Gen Intern Med. 2019 Mar;34(3):387-395. doi: 10.1007/s11606-018-4710-5. Epub 2018 Oct 31.
Opioid overdose deaths occur in civilian and military populations and are the leading cause of accidental death in the USA.
To determine whether ECHO Pain telementoring regarding best practices in pain management and safe opioid prescribing yielded significant declines in opioid prescribing.
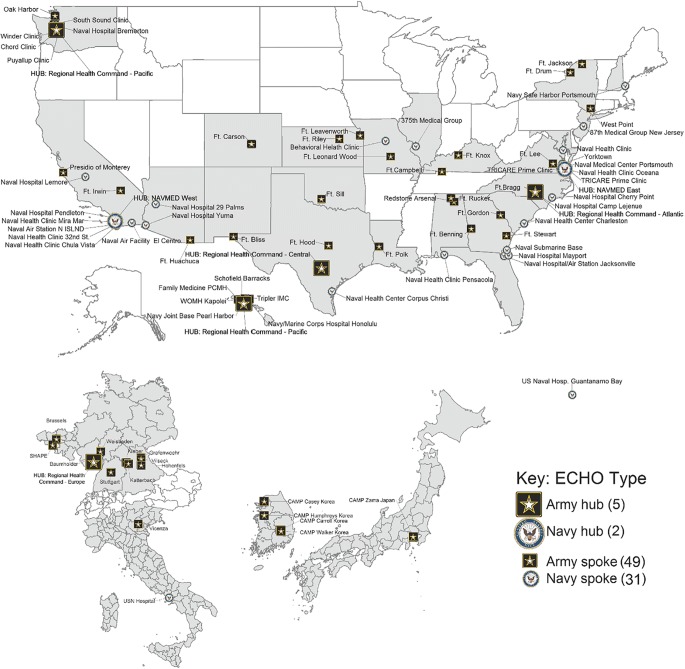
A 4-year observational cohort study at military medical treatment facilities worldwide.
Patients included 54.6% females and 46.4% males whose primary care clinicians (PCCs) opted to participate in ECHO Pain; the comparison group included 39.9% females and 60.1% males whose PCCs opted not to participate in ECHO Pain.
PCCs attended 2-h weekly Chronic Pain and Opioid Management TeleECHO Clinic (ECHO Pain), which included pain and addiction didactics, case-based learning, and evidence-based recommendations. ECHO Pain sessions were offered 46 weeks per year. Attendance ranged from 1 to 3 sessions (47.7%), 4-19 (32.1%, or > 20 (20.2%).
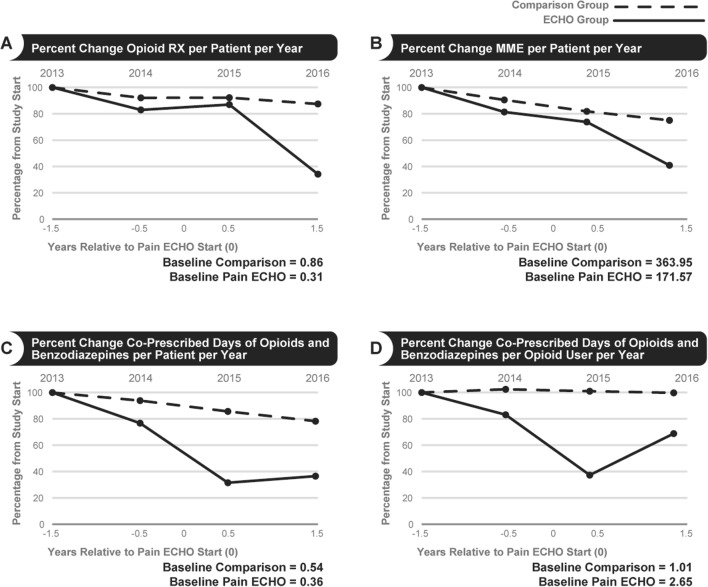
This study assessed whether clinician participation in Army and Navy Chronic Pain and Opioid Management TeleECHO Clinic (ECHO Pain) resulted in decreased prescription rates of opioid analgesics and co-prescribing of opioids and benzodiazepines. Measures included opioid prescriptions, morphine milligram equivalents (MME), and days of opioid and benzodiazepine co-prescribing per patient per year.
PCCs participating in ECHO Pain had greater percent declines than the comparison group in (a) annual opioid prescriptions per patient (- 23% vs. - 9%, P < 0.001), (b) average MME prescribed per patient/year (-28% vs. -7%, p < .02), (c) days of co-prescribed opioid and benzodiazepine per opioid user per year (-53% vs. -1%, p < .001), and (d) the number of opioid users (-20.2% vs. -8%, p < .001). Propensity scoring transformation-adjusted results were consistent with the opioid prescribing and MME results.
Patients treated by PCCs who opted to participate in ECHO Pain had greater declines in opioid-related prescriptions than patients whose PCCs opted not to participate.
阿片类药物过量死亡发生在平民和军人中,是美国意外死亡的主要原因。
确定 ECHO 疼痛远程医疗咨询在疼痛管理和安全阿片类药物处方方面的最佳实践是否导致阿片类药物处方显著减少。
一项为期 4 年的全球军事医疗设施观察性队列研究。
患者中女性占 54.6%,男性占 46.4%,他们的初级保健临床医生(PCC)选择参加 ECHO 疼痛;对照组包括女性占 39.9%,男性占 60.1%,他们的 PCC 选择不参加 ECHO 疼痛。
PCC 参加了每周 2 小时的慢性疼痛和阿片类药物管理远程 ECHO 诊所(ECHO 疼痛),包括疼痛和成瘾教学、基于案例的学习和基于证据的建议。ECHO 疼痛课程每年提供 46 周。出勤率从 1 到 3 次(47.7%),4-19 次(32.1%)或 20 次以上(20.2%)。
本研究评估了临床医生参加陆军和海军慢性疼痛和阿片类药物管理远程 ECHO 诊所(ECHO 疼痛)是否导致阿片类药物镇痛药的处方率下降以及阿片类药物和苯二氮䓬类药物的联合处方。措施包括阿片类药物处方、吗啡毫克当量(MME)以及每位患者每年阿片类药物和苯二氮䓬类药物联合处方的天数。
与对照组相比,参加 ECHO 疼痛的 PCC 患者的(a)每位患者的年度阿片类药物处方百分比下降(-23%对-9%,P<0.001),(b)每位患者/年的平均 MME 处方百分比下降(-28%对-7%,p<.02),(c)每位阿片类药物使用者/年联合开处的阿片类药物和苯二氮䓬类药物天数百分比下降(-53%对-1%,p<.001),和(d)阿片类药物使用者人数百分比下降(-20.2%对-8%,p<.001)。倾向评分转换调整后的结果与阿片类药物处方和 MME 结果一致。
选择参加 ECHO 疼痛的 PCC 治疗的患者的阿片类药物相关处方减少幅度大于选择不参加的患者。