Norfolk and Norwich University Hospital, Colney Lane, Norwich, NR4 7UY, UK.
The Hatter Cardiovascular Institute, Institute of Cardiovascular Science, University College London, London, UK.
J Cardiovasc Magn Reson. 2018 Nov 8;20(1):72. doi: 10.1186/s12968-018-0494-3.
The incidence of left ventricular (LV) thrombus formation in ST-segment elevation myocardial infarction (STEMI) patients in the current era of primary percutaneous coronary intervention (PCI) is not well established. We performed a meta-analysis to assess the actual incidence and predictors of LV thrombus by cardiovascular magnetic resonance (CMR) in STEMI treated by primary PCI.
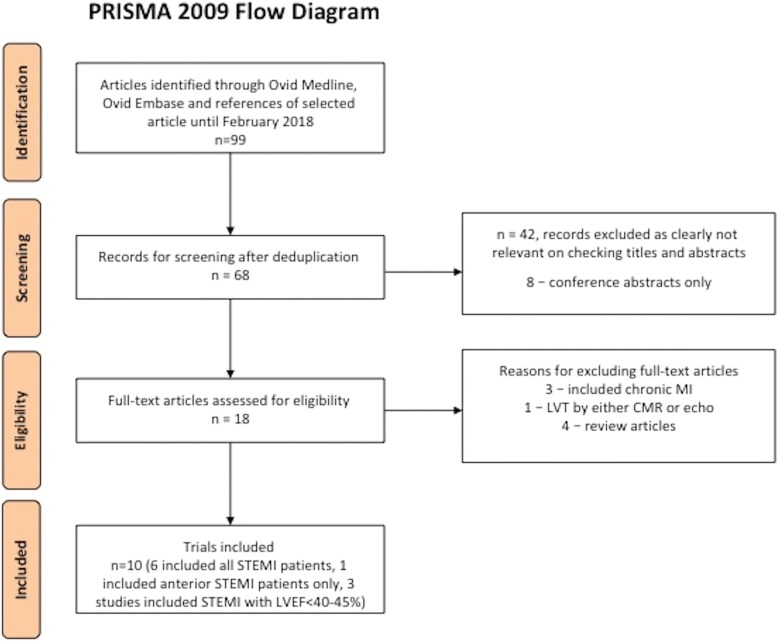
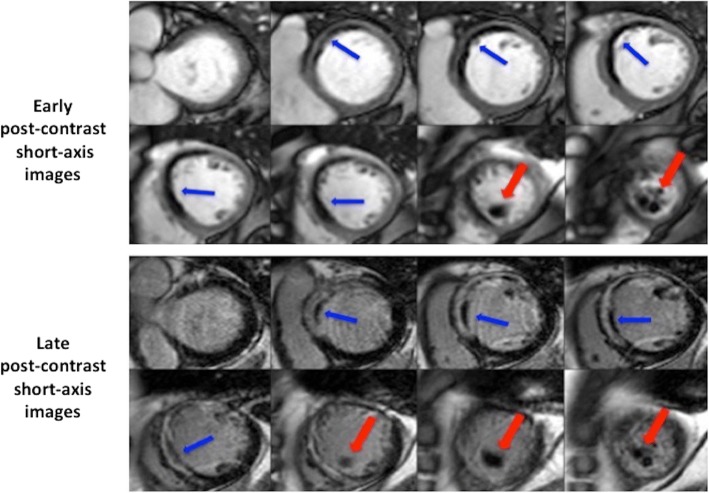
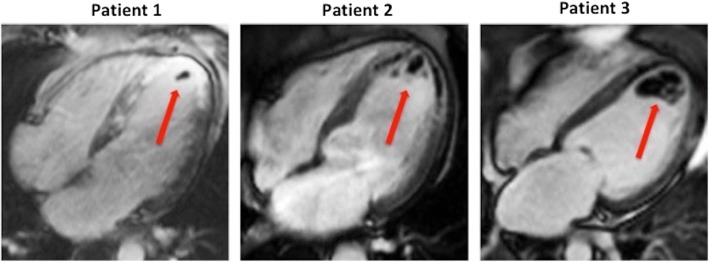
We searched MEDLINE and EMBASE databases up to February 2018. We included all studies published as a full-text article, reporting the incidence of LV thrombus by CMR within 1 month following acute STEMI in patients treated by primary PCI. A binary random-effects model was used to estimate the pooled incidence of LV thrombus. The diagnostic performance of transthoracic echocardiography (TTE) as compared with CMR was pooled to obtain the sensitivity and specificity of TTE with CMR as the gold standard. Embolic and bleeding complications of LV thrombus were also evaluated.
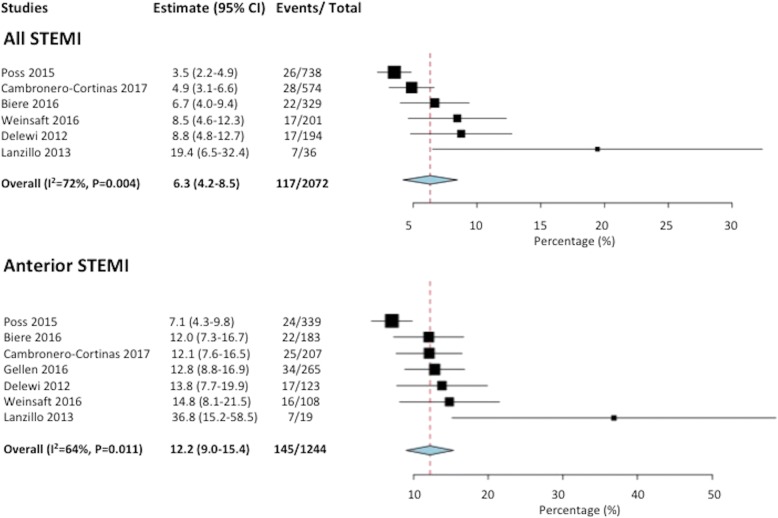
Ten studies were included in the meta-analysis. The incidence of LV thrombus by CMR in all-comer STEMI patients (n = 2072) was 6.3% with 96% of LV thrombus occurring in those with anterior STEMI (12.2% incidence). When only anterior STEMI with LVEF< 50% were considered (n = 447), the incidence of LV thrombus was 19.2%. Compared with CMR, the sensitivity of TTE to detect LV thrombus was 29% with a specificity of 98%. The sensitivity of TTE increased to 70% in those with anterior STEMI and reduced LVEF. LV thrombus resolved in 88% of cases by 3 to 6 months. After 1-2 years follow-up, the embolic complication rate was similar at 1.5% (P = 0.25) but the bleeding complication rate was significantly higher (8.8% versus 0.5%, P < 0.001) in the LV thrombus group on triple therapy when compared to the no LV thrombus group on dual antiplatelet therapy.
In the primary PCI era, CMR detection of an LV thrombus post-STEMI remains high with incidence of nearly 20% in anterior STEMI with depressed LVEF. Patients with LV thrombus treated by triple therapy had similar embolic complications but higher bleeding complications than those with no LV thrombus treated with dual antiplatelet therapy. A 3 month follow-up CMR scan to guide anticoagulation duration might help mitigate bleeding risk.
在直接经皮冠状动脉介入治疗(PCI)的时代,ST 段抬高型心肌梗死(STEMI)患者左心室(LV)血栓形成的发生率尚不清楚。我们进行了一项荟萃分析,以评估通过心血管磁共振(CMR)在直接 PCI 治疗后的 STEMI 患者中 LV 血栓的实际发生率和预测因素。
我们检索了 MEDLINE 和 EMBASE 数据库,截至 2018 年 2 月。我们纳入了所有以全文形式发表的研究,报告了在直接 PCI 治疗后的急性 STEMI 后 1 个月内通过 CMR 检测到的 LV 血栓的发生率。采用二项随机效应模型估计 LV 血栓的合并发生率。以 CMR 为金标准,汇总经胸超声心动图(TTE)与 CMR 相比的诊断性能,以获得 TTE 的敏感性和特异性。还评估了 LV 血栓的栓塞和出血并发症。
共有 10 项研究纳入荟萃分析。所有 STEMI 患者(n=2072)中,CMR 检测到的 LV 血栓发生率为 6.3%,前壁 STEMI 患者中有 96%发生 LV 血栓(发生率为 12.2%)。当仅考虑前壁 STEMI 且 LVEF<50%时(n=447),LV 血栓的发生率为 19.2%。与 CMR 相比,TTE 检测 LV 血栓的敏感性为 29%,特异性为 98%。在前壁 STEMI 且 LVEF 降低的患者中,TTE 的敏感性增加至 70%。3 至 6 个月时,88%的 LV 血栓得到溶解。在 1-2 年的随访中,LV 血栓组的栓塞并发症发生率相似,为 1.5%(P=0.25),但在 LV 血栓组接受三联治疗时,出血并发症发生率明显更高(8.8%比 0.5%,P<0.001),而在无 LV 血栓组接受双联抗血小板治疗时。
在直接 PCI 时代,CMR 检测到 STEMI 后 LV 血栓的发生率仍然很高,在前壁 STEMI 且 LVEF 降低的患者中,LV 血栓的发生率接近 20%。接受三联治疗的 LV 血栓患者的栓塞并发症发生率相似,但出血并发症发生率高于接受双联抗血小板治疗的无 LV 血栓患者。进行 3 个月的 CMR 随访以指导抗凝持续时间可能有助于降低出血风险。