Division of Imaging Sciences & Biomedical Engineering, King's College London, London, United Kingdom.
Department of Pediatrics, University of Texas Southwestern Medical Center at Dallas, United States of America.
PLoS One. 2018 Nov 8;13(11):e0205829. doi: 10.1371/journal.pone.0205829. eCollection 2018.
Cardiac output (CO) response to dobutamine can identify Alagille's syndrome (ALGS) patients at higher risk of cardiovascular complications during liver transplantation. We propose a novel patient-specific computational methodology to estimate the coronary autoregulatory responses during different hemodynamic conditions, including those experienced in a post-reperfusion syndrome (PRS), to aid cardiac risk-assessment.
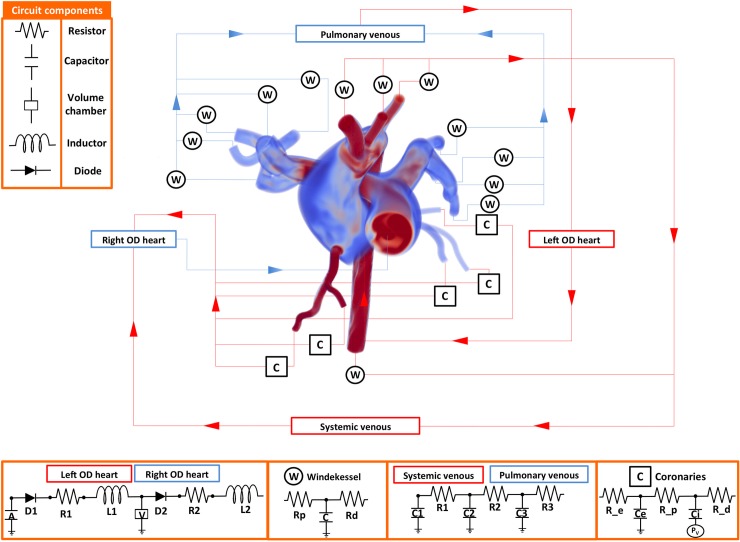
Data (pressure, flow, strain and ventricular volumes) from a 6-year-old ALGS patient undergoing catheter/dobutamine stress MRI (DSMRI) were used to parameterize a closed-loop coupled-multidomain (3D-0D) approach consisting of image-derived vascular models of pulmonary and systemic circulations and a series of 0D-lumped parameter networks (LPN) of the heart chambers and the distal arterial and venous circulations. A coronary microcirculation control model (CMCM) was designed to adjust the coronary resistance to match coronary blood flow (and thus oxygen delivery) with MVO2 requirements during Rest, Stress and a virtual PRS condition.
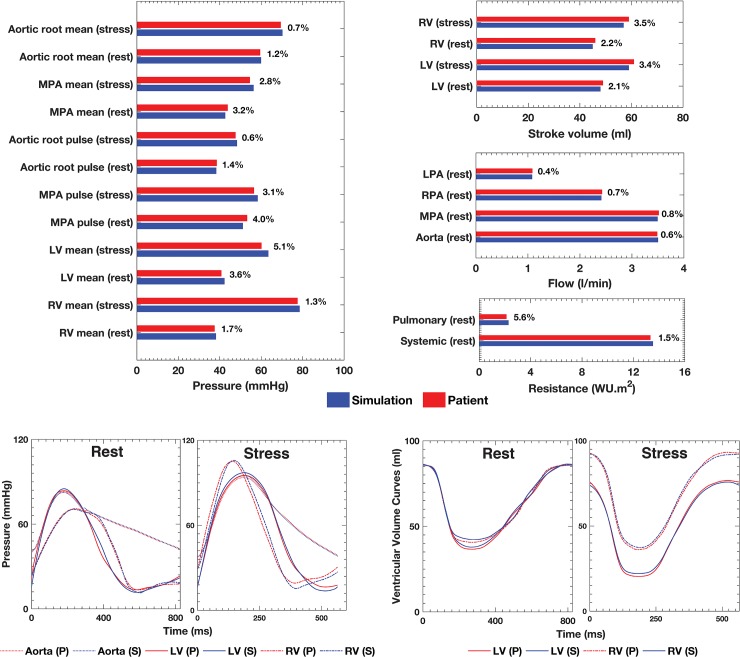
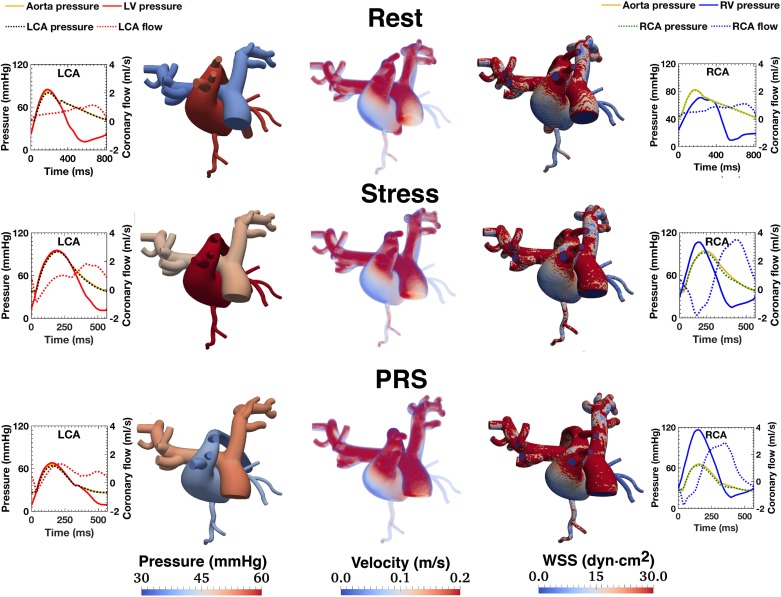
In all three simulated conditions, diastolic dominated right coronary artery (RCA) flow was observed, due to high right ventricle (RV) afterload. Despite a measured 45% increase in CO, impaired coronary flow reserve (CFR) (~1.4) at Stress was estimated by the CMCM. During modeled PRS, a marked vasodilatory response was insufficient to match RV myocardial oxygen requirements. Such exhaustion of the RCA autoregulatory response was not anticipated by the DSMRI study.
Impaired CFR undetected by DSMRI resulted in predicted myocardial ischemia in a computational model of PRS. This computational framework may identify ALGS patients at higher risk of complications during liver transplantation due to impaired coronary microvascular responses.
多巴酚丁胺的心脏输出(CO)反应可识别出在肝移植期间心血管并发症风险较高的 Alagille 综合征(ALGS)患者。我们提出了一种新的患者特异性计算方法,以估计不同血流动力学条件下的冠状动脉自动调节反应,包括在再灌注后综合征(PRS)期间经历的那些条件,以帮助进行心脏风险评估。
使用一名 6 岁 ALGS 患者的导管/多巴酚丁胺应激 MRI(DSMRI)数据(压力、流量、应变和心室容积)来参数化一个闭环耦合多域(3D-0D)方法,该方法包括肺和全身循环的图像衍生血管模型以及一系列心脏腔室和远端动脉和静脉循环的 0D 集总参数网络(LPN)。设计了一个冠状动脉微循环控制模型(CMCM),以调整冠状动脉阻力,使冠状动脉血流量(从而使氧输送)与 MVO2 在 Rest、Stress 和虚拟 PRS 条件下的需求相匹配。
在所有三种模拟条件下,由于右心室(RV)后负荷高,观察到舒张期主导的右冠状动脉(RCA)血流。尽管 CO 测量增加了 45%,但 CMCM 估计应激时的冠状动脉血流储备(CFR)(~1.4)受损。在建模的 PRS 期间,明显的血管扩张反应不足以匹配 RV 心肌的氧需求。这种 RCA 自动调节反应的衰竭是 DSMRI 研究没有预料到的。
DSMRI 未检测到的 CFR 导致 PRS 计算模型中预测的心肌缺血。这种计算框架可能会识别出由于冠状动脉微血管反应受损而在肝移植期间并发症风险较高的 ALGS 患者。