Département Biomédical et Santé Publique, Institut de Recherche en Sciences de la Santé (IRSS/CNRST), Ouagadougou, Burkina Faso.
École de Santé Publique de l'Université de Montréal (ESPUM), Montréal, Canada.
PLoS One. 2018 Nov 8;13(11):e0206978. doi: 10.1371/journal.pone.0206978. eCollection 2018.
A national subsidy policy was introduced in 2007 in Burkina Faso to improve financial accessibility to facility-based delivery. In this article, we estimated the effects of reducing user fees on institutional delivery and neonatal mortality, immediately and three years after the introduction of the policy.
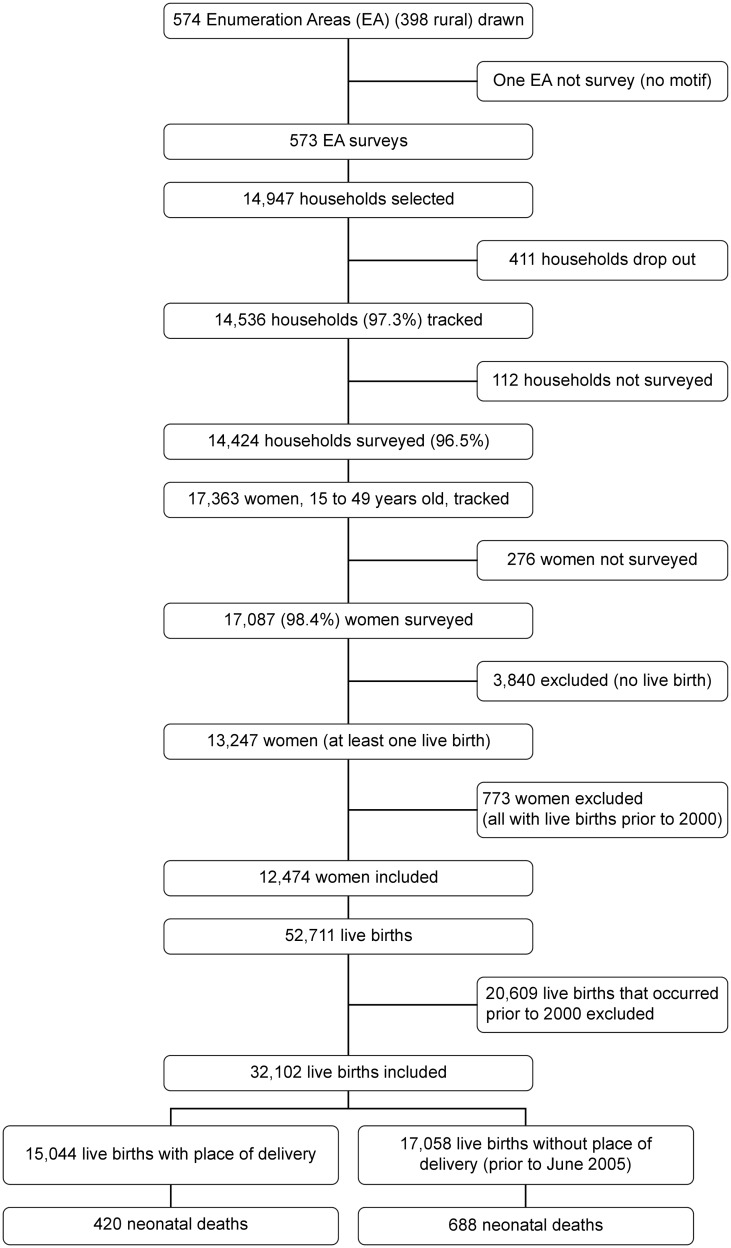
The study was based on a quasi-experimental design. We used data obtained from the 2010 Demographic and Health Survey, including survival information for 32,102 live-born infants born to 12,474 women. We used a multilevel Poisson regression model with robust variances to control for secular trends in outcomes between the period before the introduction of the policy (1 January, 2007) and the period after. In sensitivity analyses, we used two different models according to the different definitions of the period "before" and the period "after".
Immediately following its introduction, the subsidy policy was associated with increases in institutional deliveries by 4% (RR = 1.04, 95% CI: 0.98-1.10) in urban areas and by 12% (RR = 1.12, 95% CI: 1.04-1.20) in rural areas. The results showed similar patterns in sensitivity analyses. This effect was particularly marked among rural clusters with low institutional delivery rates at baseline (RR = 1.44, 95% CI: 1.33-1.55). It was persistent for 42 months after the introduction of the policy but these increases were not statistically significant. At 42 months, the delivery rates had increased by 26% in rural areas (RR = 1.26; 95% CI: 0.86-1.86) and 13% (RR = 1.13; 95% CI: 0.88-1.46) in urban areas. There was no evidence of a significant decrease in neonatal mortality rates.
The delivery subsidy implemented in Burkina Faso is associated with short-term increases in health facility deliveries. This policy has been particularly beneficial for rural households.
2007 年,布基纳法索出台了一项国家补贴政策,以提高获得医疗机构分娩服务的财政可及性。本文旨在评估该政策对医疗机构分娩和新生儿死亡率的影响,包括政策出台后即刻和三年后的影响。
本研究采用准实验设计。我们使用了 2010 年人口与健康调查获得的数据,包括 12474 名产妇所生 32102 名活产婴儿的生存信息。我们采用了多水平泊松回归模型,使用稳健方差来控制政策出台前后(2007 年 1 月 1 日)结果的时间趋势。在敏感性分析中,我们根据“之前”和“之后”两个时期的不同定义,使用了两种不同的模型。
政策出台后即刻,城市地区医疗机构分娩率增加了 4%(RR=1.04,95%CI:0.98-1.10),农村地区增加了 12%(RR=1.12,95%CI:1.04-1.20)。敏感性分析结果显示出相似的模式。对于基线时医疗机构分娩率较低的农村地区,这种效果更为显著(RR=1.44,95%CI:1.33-1.55)。这种影响持续了 42 个月,但没有统计学意义。在 42 个月时,农村地区的分娩率增加了 26%(RR=1.26;95%CI:0.86-1.86),城市地区增加了 13%(RR=1.13;95%CI:0.88-1.46)。没有证据表明新生儿死亡率有显著下降。
布基纳法索实施的分娩补贴与短期医疗机构分娩率的增加有关。该政策对农村家庭尤其有益。