1 Department of Radiology, Memorial Sloan Kettering Cancer Center, 1275 York Ave, New York, NY 10065.
2 Department of Radiology, Hospital Sírio-Libanês, São Paulo, Brazil.
AJR Am J Roentgenol. 2019 Jan;212(1):94-102. doi: 10.2214/AJR.18.19928. Epub 2018 Nov 13.
The purpose of the present study is to evaluate the diagnostic performance of and interreader agreement for CT colonography (CTC) in the local staging of colon cancer, with emphasis given to the FOxTROT (Fluoropyrimidine, Oxaliplatin, and Targeted-Receptor pre-Operative Therapy [Panitumumab]) trial inclusion criteria, which propose a new tailored treatment paradigm for colon cancer that uses neoadjuvant therapy for patients with a high-risk of locoregional disease as determined by imaging.
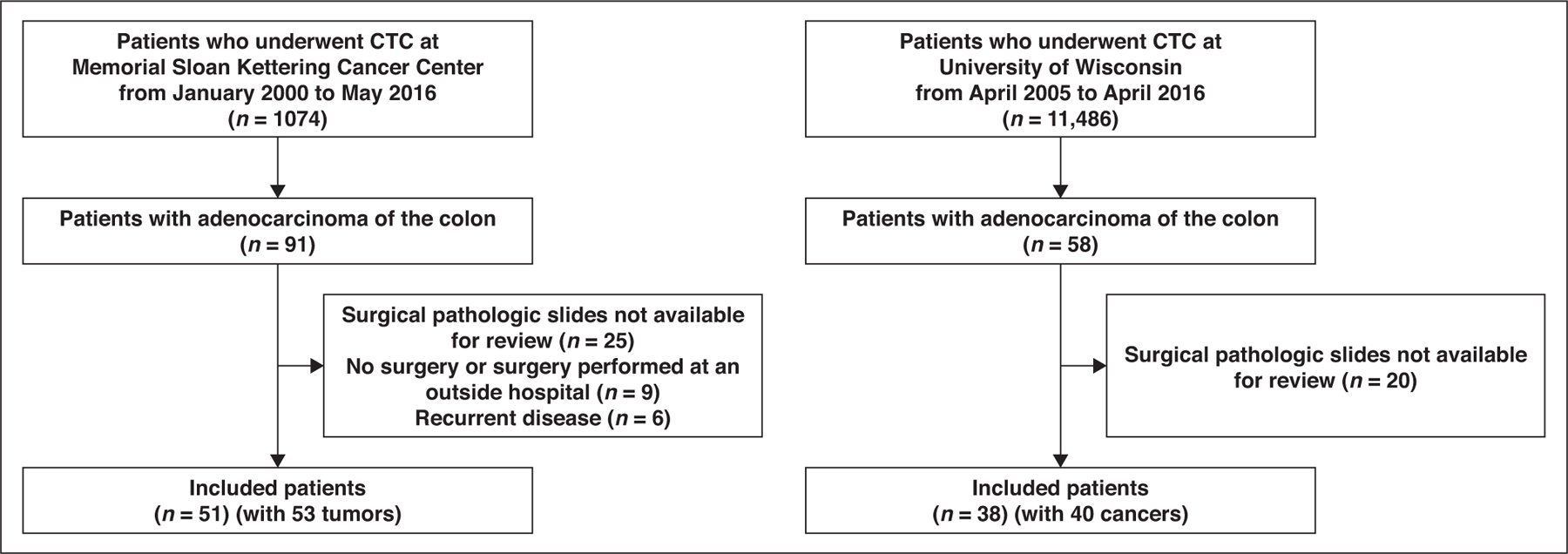
This biinstitutional retrospective study involved 89 patients (with 93 tumors) who had colon cancer and underwent presurgical CTC. Two radiologists reviewed the CTC studies for local staging, including measurement of the tumor beyond the muscularis propria on a true orthogonal plane. Histopathologic findings for surgical colectomy specimens served as the reference standard for local pathologic staging. The sensitivity, specificity, positive predictive value, and negative predictive value for local determination of the T category, N category, and extramural vascular invasion (EMVI) were calculated separately for each reader. High-risk T category tumors were the same as those as used in the FOxTROT trial. Interreader agreement was assessed using the kappa statistic.
Thirty-five of 93 tumors (37.6%) were histologically classified as high-risk tumors (T3c, T3d, or T4 tumors). The interreader agreement was substantial (κ = 0.68) for classifying high-risk tumors with the use of CTC, moderate for differentiating N0 from N1 and N2 (κ = 0.44), and slight for detecting EMVI (κ = 0.15). The diagnostic statistics for CTC for the two readers were as follows: for detection of high-risk tumors, sensitivity was 65.7% and 82.9%, and specificity was 81.0% and 87.9%; for detection of N category-positive disease, sensitivity was 50.9% and 69.8%, and specificity was 50.0% and 72.5%; and for detection of EMVI, sensitivity was 18.2% and 66.7%, and specificity was 60.0% and 91.7%.
The present study shows that CTC might be a feasible imaging modality for preoperative local staging of higher-risk colon cancers for which neoadjuvant chemotherapy is more suitable on the basis of the FOxTROT trial criteria. However, further studies are required to allow a better generalization of our results.
本研究旨在评估 CT 结肠成像(CTC)在结肠癌局部分期中的诊断性能和读者间一致性,重点关注 FOxTROT(氟嘧啶、奥沙利铂和靶向受体术前治疗[帕尼单抗])试验纳入标准,该标准提出了一种新的结肠癌治疗模式,即对影像学检查显示局部疾病高风险的患者使用新辅助治疗。
这项双机构回顾性研究纳入了 89 名(93 个肿瘤)患有结肠癌并接受术前 CTC 检查的患者。两名放射科医生对 CTC 研究进行了局部分期评估,包括在真实正交平面上测量肿瘤超出肌层。手术切除标本的组织病理学检查结果作为局部病理分期的参考标准。分别计算每位读者对 T 分期、N 分期和外膜血管侵犯(EMVI)的局部 T 分期、N 分期和外膜血管侵犯(EMVI)的敏感性、特异性、阳性预测值和阴性预测值。高危 T 期肿瘤与 FOxTROT 试验相同。使用κ 统计评估读者间的一致性。
93 个肿瘤中有 35 个(37.6%)组织学上被归类为高危肿瘤(T3c、T3d 或 T4 肿瘤)。使用 CTC 对高危肿瘤进行分类的读者间一致性为中等(κ=0.68),对 N0、N1 和 N2 进行分类的读者间一致性为中度(κ=0.44),对检测 EMVI 的读者间一致性为轻微(κ=0.15)。两位读者对 CTC 的诊断统计结果如下:对高危肿瘤的检测,敏感性为 65.7%和 82.9%,特异性为 81.0%和 87.9%;对 N 期阳性疾病的检测,敏感性为 50.9%和 69.8%,特异性为 50.0%和 72.5%;对 EMVI 的检测,敏感性为 18.2%和 66.7%,特异性为 60.0%和 91.7%。
本研究表明,CTC 可能是一种可行的影像学方法,可用于基于 FOxTROT 试验标准更适合新辅助化疗的高危结肠癌的术前局部分期。然而,需要进一步的研究来更好地推广我们的结果。