The Farr Institute of Health Informatics Research, Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, UK.
Department of Mathematics and Statistics, University of Strathclyde, Glasgow, UK.
Br J Clin Pharmacol. 2019 Feb;85(2):422-431. doi: 10.1111/bcp.13814. Epub 2018 Dec 18.
The aim of this study was to compare the clinical effectiveness and safety of direct oral anticoagulants (DOACs) in patients with atrial fibrillation (AF) in routine clinical practice.
This retrospective cohort study used linked administrative data. The study population (n = 14 577) included patients with a diagnosis of AF (confirmed in hospital) who initiated DOAC treatment in Scotland between August 2011 and December 2015. Multivariate Cox proportional hazard models were used to estimate hazard ratios of thromboembolic events, mortality and bleeding events.
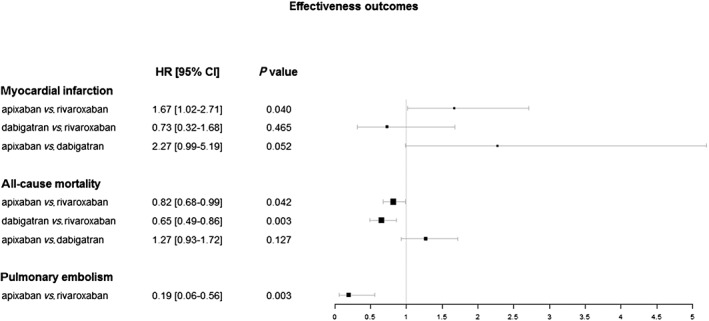
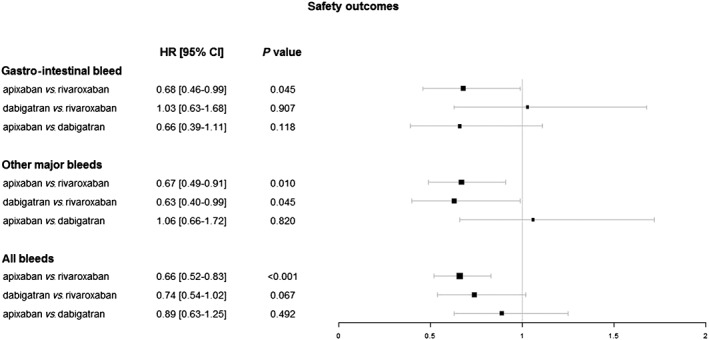
No differences between the DOACs were observed with regard to the risk of stroke, systemic embolism or cardiovascular death. In contrast, the risk of myocardial infarction was higher among patients prescribed apixaban in comparison to those on rivaroxaban (HR 1.67, 95% CI 1.02-2.71), and all-cause mortality was higher among rivaroxaban patients in contrast to both apixaban (1.22 [1.01-1.47]) and dabigatran (1.55 [1.16-2.05]) patients; rivaroxaban patients also had a higher risk of pulmonary embolism than apixaban patients (5.27 [1.79-15.53]). The risk of other major bleeds was higher among rivaroxaban patients compared to apixaban (1.50 [1.10-2.03]) and dabigatran (1.58 [1.01-2.48]) patients; the risks of gastrointestinal bleeds and overall bleeding were higher among rivaroxaban patients than among apixaban patients (1.48 [1.01-2.16] and 1.52 [1.21-1.92], respectively).
All DOACs were similarly effective in preventing strokes and systemic embolisms, while patients being treated with rivaroxaban exhibited the highest bleeding risks. Observed differences in the risks of all-cause mortality, myocardial infarction and pulmonary embolism warrant further research.
本研究旨在比较直接口服抗凝剂(DOAC)在常规临床实践中治疗房颤(AF)患者的临床疗效和安全性。
这是一项回顾性队列研究,使用了关联的行政数据。研究人群(n=14577)包括 2011 年 8 月至 2015 年 12 月期间在苏格兰接受 DOAC 治疗且有 AF(在医院确诊)诊断的患者。采用多变量 Cox 比例风险模型估计血栓栓塞事件、死亡率和出血事件的风险比。
在卒中、全身性栓塞或心血管死亡风险方面,不同 DOAC 之间无差异。相比之下,与 rivaroxaban 相比,接受 apixaban 治疗的患者心肌梗死风险更高(HR 1.67,95%CI 1.02-2.71),与 apixaban(1.22 [1.01-1.47])和 dabigatran(1.55 [1.16-2.05])患者相比,rivaroxaban 患者的全因死亡率更高;与 apixaban 患者相比,rivaroxaban 患者的肺栓塞风险更高(5.27 [1.79-15.53])。与 apixaban 相比,rivaroxaban 患者发生其他主要出血的风险更高(1.50 [1.10-2.03])和 dabigatran(1.58 [1.01-2.48]);与 apixaban 患者相比,rivaroxaban 患者发生胃肠道出血和总体出血的风险更高(1.48 [1.01-2.16] 和 1.52 [1.21-1.92])。
所有 DOAC 在预防卒中及全身性栓塞方面同样有效,而 rivaroxaban 治疗患者的出血风险最高。观察到的全因死亡率、心肌梗死和肺栓塞风险差异需要进一步研究。