Health Care Division, Health and Counseling Center, Osaka University, Toyonaka, Osaka, Japan.
Department of Nephrology, Osaka University Graduate School of Medicine, Suita, Osaka, Japan.
Clin J Am Soc Nephrol. 2018 Dec 7;13(12):1825-1832. doi: 10.2215/CJN.01340118. Epub 2018 Nov 15.
Shorter or longer sleep duration and poor sleep quality are risk factors for numerous cardio-metabolic diseases, cardiovascular disease, and mortality in subjects with normal kidney function. The association of sleep duration and sleep quality with health outcomes in patients with CKD remains uncertain.
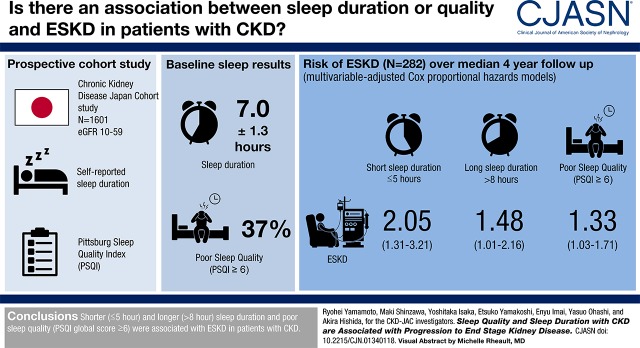
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: A 4-year prospective cohort study in 17 nephrology centers in Japan, the CKD Japan Cohort (CKD-JAC) Study, assessed an association of self-reported sleep duration and sleep quality, on the basis of the Pittsburgh Sleep Quality Index (PSQI) questionnaire, with incidence of ESKD in 1601 patients with eGFR 10-59 ml/min per 1.73 m using multivariable-adjusted Cox proportional hazards models.
Baseline sleep duration and PSQI global score for the 1601 patients were mean±SD 7.0±1.3 hours and median 4 (interquartile range, 3-7), respectively. Poor sleep quality (PSQI global score ≥6) was common (=588 [37%]). During a median of 4.0 (2.6-4.3) years of the follow-up period, 282 (18%) patients progressed to ESKD. After adjusting for age, sex, eGFR, urinary albumin excretion, smoking status, body mass index, history of diabetes and cardiovascular disease, systolic BP, blockade of the renin-angiotensin system, use of hypnotics, and Beck depression inventory score, both shorter (≤5 hour) and longer (>8 hour) sleep duration were associated with ESKD (adjusted hazard ratios [95% confidence intervals] for ≤5.0, 5.1-6.0, 6.1-7.0, 7.1-8.0, and ≥8.0 hours were 2.05 [1.31 to3.21], 0.98 [0.67 to 1.44], 1.00 [reference], 1.22 [0.89 to 1.66], and 1.48 [1.01 to 2.16]), suggesting a U-shaped relationship between sleep duration and ESKD. PSQI global score ≥6 was also associated with incidence of ESKD (adjusted hazard ratios [95% confidence intervals] for PSQI global score ≤5 and ≥6 were 1.00 [reference] and 1.33 [1.03 to 1.71]).
Shorter (≤5 hour) and longer (>8 hour) sleep duration and poor sleep quality (PSQI global score ≥6) were associated with ESKD in patients with CKD.
睡眠时长较短或较长,以及睡眠质量较差,是肾功能正常人群中发生多种心血管代谢疾病、心血管疾病和死亡的风险因素。睡眠时长和睡眠质量与慢性肾脏病(CKD)患者健康结果之间的关联尚不确定。
这是一项在日本 17 个肾病中心开展的、为期 4 年的前瞻性队列研究,即 CKD 日本队列(CKD-JAC)研究,通过多变量调整的 Cox 比例风险模型,评估了 1601 例 eGFR 为 10-59ml/min/1.73m2 的患者自我报告的睡眠时长和睡眠质量(基于匹兹堡睡眠质量指数(PSQI)问卷)与终末期肾病(ESKD)发生的相关性。
在 1601 例患者中,基线睡眠时长和 PSQI 总分的平均值±标准差分别为 7.0±1.3 小时和中位数 4(四分位距,3-7)。睡眠质量较差(PSQI 总分≥6)很常见(=588[37%])。在中位随访 4.0(2.6-4.3)年后,282 例(18%)患者进展为 ESKD。在调整年龄、性别、eGFR、尿白蛋白排泄率、吸烟状况、体重指数、糖尿病和心血管疾病史、收缩压、肾素-血管紧张素系统阻断、催眠药物使用以及贝克抑郁量表评分后,睡眠时长较短(≤5 小时)和较长(>8 小时)与 ESKD 相关(≤5.0、5.1-6.0、6.1-7.0、7.1-8.0 和≥8.0 小时的校正风险比[95%置信区间]分别为 2.05[1.31 至 3.21]、0.98[0.67 至 1.44]、1.00[参考]、1.22[0.89 至 1.66]和 1.48[1.01 至 2.16]),提示睡眠时长与 ESKD 之间呈 U 形关系。PSQI 总分≥6 也与 ESKD 发生率相关(PSQI 总分≤5 和≥6 的校正风险比[95%置信区间]分别为 1.00[参考]和 1.33[1.03 至 1.71])。
较短(≤5 小时)和较长(>8 小时)的睡眠时长以及较差的睡眠质量(PSQI 总分≥6)与 CKD 患者的 ESKD 相关。