Department of Surgical Intensive Care Unit, Beijing Chao-yang Hospital, 8 Gongren Tiyuchang Nanlu, Chaoyang District, Beijing, 100020, China.
Crit Care. 2018 Nov 16;22(1):305. doi: 10.1186/s13054-018-2232-5.
Acute kidney injury (AKI) is associated with high morbidity and mortality in surgical patients. Nonrecovery from AKI may increase mortality and early risk stratification seems key to improving clinical outcomes. The aim of the current study was to explore and validate the value of endostatin for predicting failure to recover from AKI.
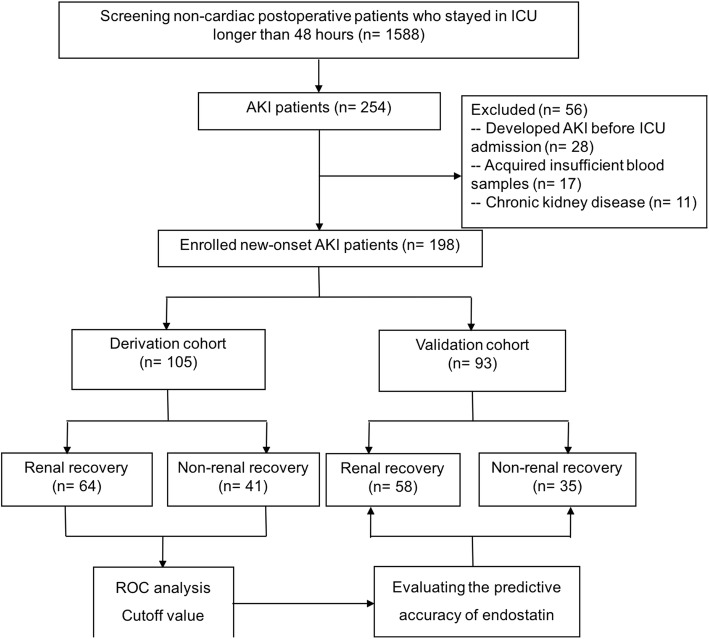
We conducted a prospective cohort study of 198 patients without known chronic kidney disease who underwent noncardiac major surgery and developed new-onset AKI in the first 48 h after admission to the ICU. The biomarkers of plasma endostatin, neutrophil gelatinase-associated lipocalin (NGAL) and cystatin C were detected immediately after AKI diagnosis. The primary endpoint was nonrecovery from AKI (within 7 days). Cutoff values of the biomarkers for predicting nonrecovery were determined in a derivation cohort (105 AKI patients). Predictive accuracy was then analyzed in a validation cohort (93 AKI patients).
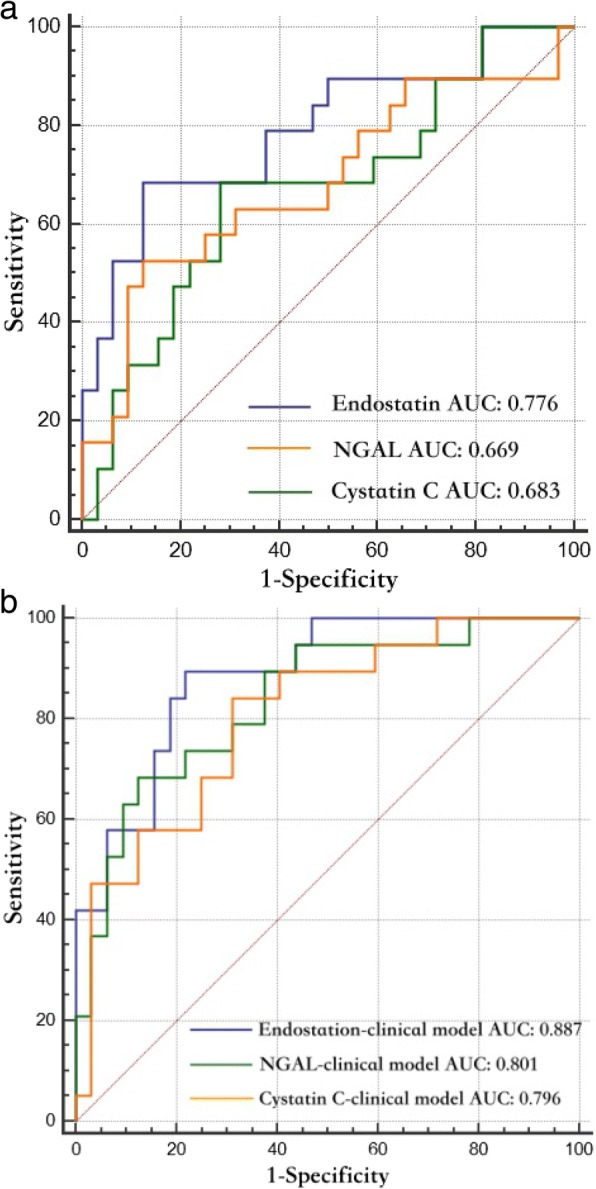
Seventy-six of 198 (38.4%) patients failed to recover from AKI onset, with 41 in the derivation cohort and 35 in the validation cohort. Compared with NGAL and cystatin C, endostatin showed a better prediction for nonrecovery, with an area under the receiver operating characteristic curve (AUC) of 0.776 (95% confidence interval (CI) 0.654-0.892, p < 0.001) and an optimal cutoff value of 63.7 ng/ml. The predictive ability for nonrecovery was greatly improved by the prediction model combining endostatin with clinical risk factors of Sequential Organ Failure Assessment (SOFA) score and AKI classification, with an AUC of 0.887 (95% CI 0.766-0.958, p < 0.001). The value of the endostatin-clinical risk prediction model was superior to the NGAL-clinical risk and cystatin C-clinical risk prediction models in predicting failure to recover from AKI, which was supported by net reclassification improvement and integrated discrimination improvement. Further, the endostatin-clinical risk prediction model achieved sensitivity and specificity of 94.6% (76.8-99.1) and 72.7% (57.2-85.0), respectively, when validated in the validation cohort.
Plasma endostatin shows a useful value for predicting failure to recover from AKI. The predictive ability can be greatly improved when endostatin is combined with the SOFA score and AKI classification.
急性肾损伤(AKI)与外科患者的高发病率和死亡率相关。AKI 无法恢复可能会增加死亡率,早期风险分层似乎是改善临床结局的关键。本研究的目的是探讨并验证内皮抑素预测 AKI 恢复失败的价值。
我们进行了一项前瞻性队列研究,纳入了 198 名无已知慢性肾脏病且在 ICU 入院后 48 小时内新发 AKI 的非心脏大手术患者。在 AKI 诊断后立即检测血浆内皮抑素、中性粒细胞明胶酶相关脂质运载蛋白(NGAL)和胱抑素 C 的生物标志物。主要终点为 AKI 恢复失败(7 天内)。在推导队列(105 例 AKI 患者)中确定生物标志物预测恢复失败的截断值。然后在验证队列(93 例 AKI 患者)中分析预测准确性。
198 例患者中有 76 例(38.4%)未能从 AKI 发作中恢复,其中 41 例在推导队列中,35 例在验证队列中。与 NGAL 和胱抑素 C 相比,内皮抑素对恢复失败的预测效果更好,其受试者工作特征曲线下面积(AUC)为 0.776(95%置信区间(CI)为 0.654-0.892,p<0.001),最佳截断值为 63.7ng/ml。内皮抑素与序贯器官衰竭评估(SOFA)评分和 AKI 分类的临床危险因素相结合的预测模型,极大地提高了对恢复失败的预测能力,AUC 为 0.887(95%CI 0.766-0.958,p<0.001)。内皮抑素-临床风险预测模型在预测 AKI 恢复失败方面优于 NGAL-临床风险和胱抑素 C-临床风险预测模型,这得到了净重新分类改善和综合判别改善的支持。此外,当在验证队列中验证时,内皮抑素-临床风险预测模型的灵敏度和特异性分别为 94.6%(76.8-99.1)和 72.7%(57.2-85.0)。
血浆内皮抑素对预测 AKI 恢复失败具有一定价值。当内皮抑素与 SOFA 评分和 AKI 分类相结合时,预测能力可以得到极大提高。