Farber Nicholas J, Rivera-Núñez Zorimar, Kim Sinae, Shinder Brian, Radadia Kushan, Sterling Joshua, Modi Parth K, Goyal Sharad, Parikh Rahul, Mayer Tina M, Weiss Robert E, Kim Isaac Y, Elsamra Sammy E, Jang Thomas L, Singer Eric A
Section of Urologic Oncology, Rutgers Cancer Institute of New Jersey, New Brunswick, NJ.
Department of Radiation Oncology, Rutgers Cancer Institute of New Jersey, New Brunswick, NJ.
Urol Oncol. 2019 Jan;37(1):26-32. doi: 10.1016/j.urolonc.2018.10.004. Epub 2018 Nov 13.
Lymph node (LN) involvement in renal cell carcinoma (RCC) is associated with a poor prognosis. While lymph node dissection (LND) may provide diagnostic information, its therapeutic benefit remains controversial. Thus, the aim of our study is to analyze survival outcomes after LND for nonmetastatic RCC and to characterize contemporary practice patterns.
The National Cancer Database was queried for patients with nonmetastatic RCC who underwent either partial or radical nephrectomy from 2010 to 2014. A total of 11,867 underwent surgery and LND. Chi-square tests were used to examine differences in patient demographics. To minimize selection bias, propensity score matching (PSM) was used to select one control for each LND case (n = 19,500). Cox regression analyses were conducted to examine overall survival (OS) in patients who received LND compared to those who did not.
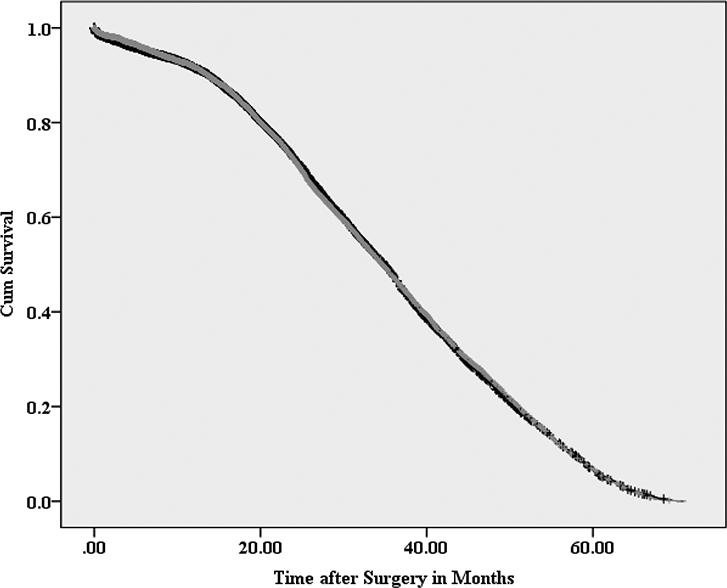
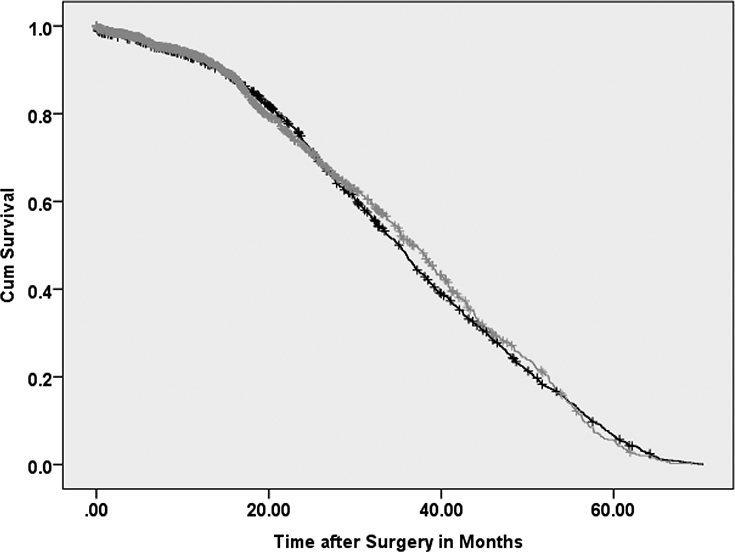
Of all patients undergoing LND for RCC (n = 11,867), 5%, 23%, 31%, 47% were performed for tumors of clinical T stage 1, 2, 3, and 4, respectively. Proportions of LND have not significantly changed from 2010 to 2014. No significant improvement in median OS for patients undergoing LND compared to no LND was shown (34.7 vs. 34.9 months, respectively; P = 0.98). Similarly, no significant improvement in median OS was found for clinically LN positive patients undergoing LND compared to no LND (P = 0.90). On Cox regression analysis, LND dissection was not associated with an OS benefit (hazard ratio: 1.00; 95% confidence interval 0.97 to 1.04).
Among all RCC patients, LNDs are often performed for low stage disease, suggesting a potential overutilization of LND. No OS benefit was seen in any subgroup of patients undergoing LND. Further investigation is needed to determine which patient populations may benefit most from LND.
肾细胞癌(RCC)出现淋巴结(LN)转移与预后不良相关。虽然淋巴结清扫术(LND)可能提供诊断信息,但其治疗益处仍存在争议。因此,我们研究的目的是分析非转移性RCC患者接受LND后的生存结果,并描述当代的实践模式。
查询国家癌症数据库中2010年至2014年接受部分或根治性肾切除术的非转移性RCC患者。共有11,867例患者接受了手术和LND。采用卡方检验来检查患者人口统计学特征的差异。为了尽量减少选择偏倚,使用倾向评分匹配(PSM)为每个LND病例选择一个对照(n = 19,500)。进行Cox回归分析,以检查接受LND的患者与未接受LND的患者的总生存期(OS)。
在所有接受RCC的LND患者(n = 11,867)中,分别有5%、23%、31%、47%的患者因临床T分期为1、2、3、4期的肿瘤而进行LND。从2010年到2014年,LND的比例没有显著变化。与未接受LND的患者相比,接受LND的患者的中位OS没有显著改善(分别为34.7个月和34.9个月;P = 0.98)。同样,与未接受LND的患者相比,接受LND的临床LN阳性患者的中位OS也没有显著改善(P = 0.90)。在Cox回归分析中,LND与OS获益无关(风险比:1.00;95%置信区间0.97至1.04)。
在所有RCC患者中,LND通常用于低分期疾病,这表明LND可能存在过度使用的情况。在接受LND的任何亚组患者中均未观察到OS获益。需要进一步研究以确定哪些患者群体可能从LND中获益最大。