Department of Brain Repair and Rehabilitation, UCL Queen Square Institute of Neurology and the National Hospital for Neurology and Neurosurgery UCL Stroke Research Centre, London, UK.
Department of Statistical Science, University College London, London, UK.
J Neurol Neurosurg Psychiatry. 2019 Mar;90(3):320-325. doi: 10.1136/jnnp-2018-318890. Epub 2018 Nov 19.
The optimal time to start oral anticoagulant (OAC) in patients with ischaemic stroke due to non-valvular atrial fibrillation (AF) is unknown. We reviewed OAC timing in relation to 90-day clinical outcomes as a post hoc analysis from a prospective multicentre observational study.
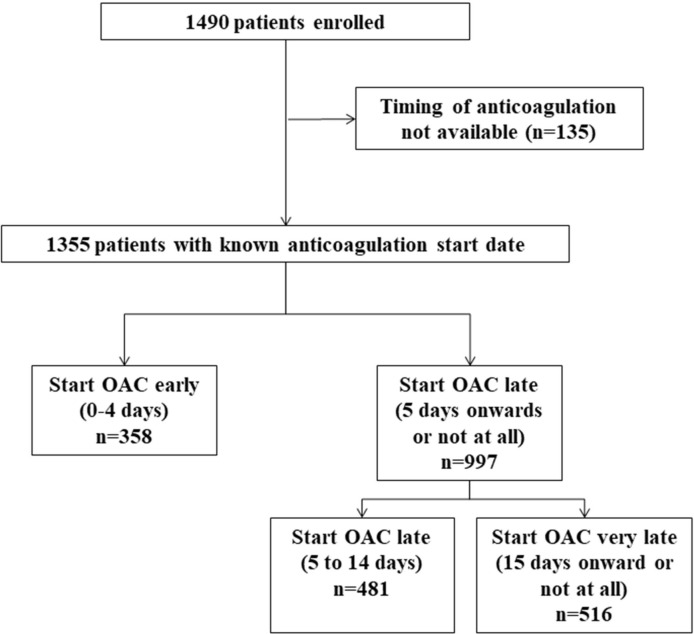
We included patients with data on time to initiation of OAC from CROMIS-2 (Clinical Relevence Of Microbleeds In Stroke-2), a prospective observational inception cohort study of 1490 patients with ischaemic stroke or transient ischaemic attack (TIA) and AF treated with OAC. The primary outcome was the composite outcome of TIA, stroke (ischaemic stroke or intracranial haemorrhage) or death within 90 days of the qualifying stroke or TIA. We performed adjusted logistic regression analyses to compare early (0-4 days) and later (≥5 days or never started) OAC initiation.
We included 1355 patients, mean age 76 (SD 10), 580 (43%) women. OAC was started early in 358 (26%) patients and later (or not at all) in 997 (74%) patients. The event rate within 90 days was 48/997 (5%) in the late-OAC group (2 intracranial haemorrhages, 18 ischaemic strokes or TIAs and 31 deaths (three deaths were as a result of new ischaemic strokes)) versus 7/358 (2%) in the early-OAC group (5 ischaemic strokes or TIAs and 2 deaths). In adjusted analyses, late OAC was not associated with the composite outcome (adjusted OR 1.17, 95% CI 0.48 to 2.84, p=0.736).
In adjusted analyses, early OAC after acute ischaemic stroke or TIA associated with AF was not associated with a difference in the rate of the composite outcome of stroke, TIA or death at 90 days, compared with late OAC. However, despite adjustment for important baseline factors, patients selected for early OAC and late OAC might still have differed in important respects; evaluation of OAC timing in adequately powered randomised trials is required.
NCT02513316.
非瓣膜性心房颤动(AF)导致的缺血性脑卒中患者开始口服抗凝剂(OAC)的最佳时间尚不清楚。我们对一项前瞻性多中心观察性研究(CROMIS-2)中与 90 天临床结局相关的 OAC 时机进行了回顾性分析。
我们纳入了 CROMIS-2(卒中 2 中微出血的临床相关性)研究中具有 OAC 起始时间数据的患者,该研究为前瞻性观察性起始队列研究,纳入了 1490 例缺血性卒中和短暂性脑缺血发作(TIA)合并 AF 患者,接受 OAC 治疗。主要结局是 90 天内 TIA、卒中和死亡(缺血性卒中和颅内出血)的复合结局。我们进行了调整后的逻辑回归分析,以比较早期(0-4 天)和晚期(≥5 天或从未开始)OAC 起始。
我们纳入了 1355 例患者,平均年龄 76(10)岁,580 例(43%)为女性。358 例(26%)患者早期开始 OAC,997 例(74%)患者晚期(或根本未开始)开始 OAC。997 例晚期 OAC 组中,90 天内的事件发生率为 48/997(5%)(2 例颅内出血、18 例缺血性卒中和 TIA 和 31 例死亡(3 例死亡是新发缺血性卒中所致)),而 358 例早期 OAC 组中,事件发生率为 7/358(2%)(5 例缺血性卒中和 TIA 和 2 例死亡)。调整分析后,晚期 OAC 与复合结局无关(调整后的 OR 1.17,95%CI 0.48 至 2.84,p=0.736)。
在调整分析中,与急性缺血性卒中和 TIA 合并 AF 相关的早期 OAC 与 90 天时卒中、TIA 或死亡的复合结局发生率无差异,与晚期 OAC 相比。然而,尽管对重要的基线因素进行了调整,选择早期 OAC 和晚期 OAC 的患者在重要方面可能仍存在差异;需要在充分的随机试验中评估 OAC 时机。
NCT02513316。