Department of Neurology and Stroke Center, University Hospital Basel and University of Basel, Basel, Switzerland.
Neurology and Neurorehabilitation, University Hospital for Geriatric Medicine Felix Platter, University of Basel, Basel, Switzerland.
Ann Neurol. 2023 Jul;94(1):43-54. doi: 10.1002/ana.26654. Epub 2023 Apr 13.
Atrial fibrillation (AF) known before ischemic stroke (KAF) has been postulated to be an independent category with a recurrence risk higher than that of AF detected after stroke (AFDAS). However, it is unknown whether this risk difference is confounded by pre-existing anticoagulation, which is most common in KAF and also indicates a high ischemic stroke recurrence risk.
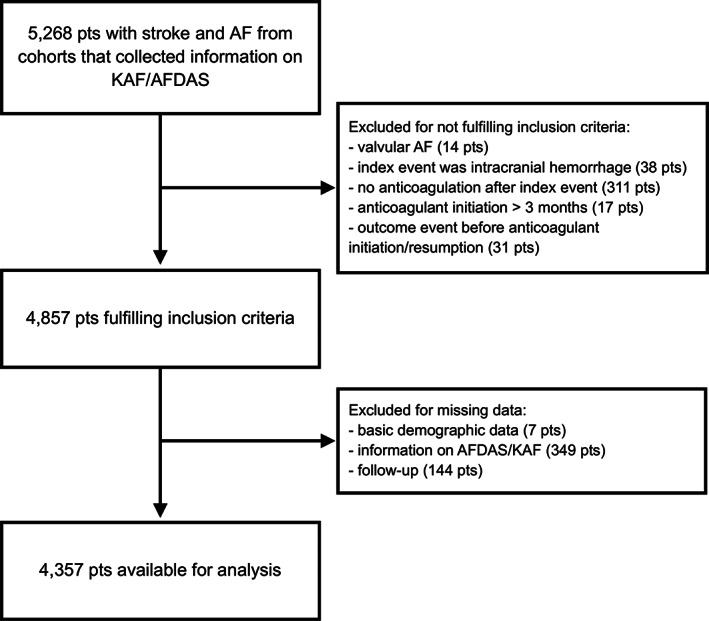
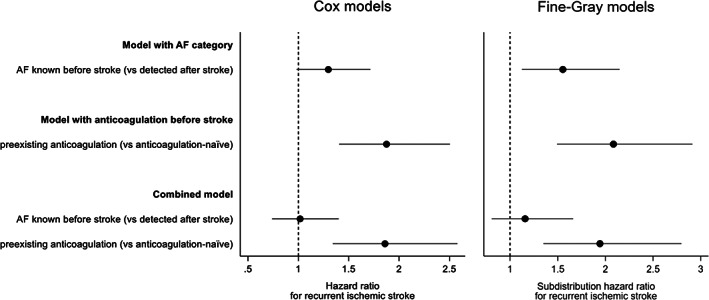
Individual patient data analysis from 5 prospective cohorts of anticoagulated patients following AF-associated ischemic stroke. We compared the primary (ischemic stroke recurrence) and secondary outcome (all-cause death) among patients with AFDAS versus KAF and among anticoagulation-naïve versus previously anticoagulated patients using multivariable Cox, Fine-Gray models, and goodness-of-fit statistics to investigate the relative independent prognostic importance of AF-category and pre-existing anticoagulation.
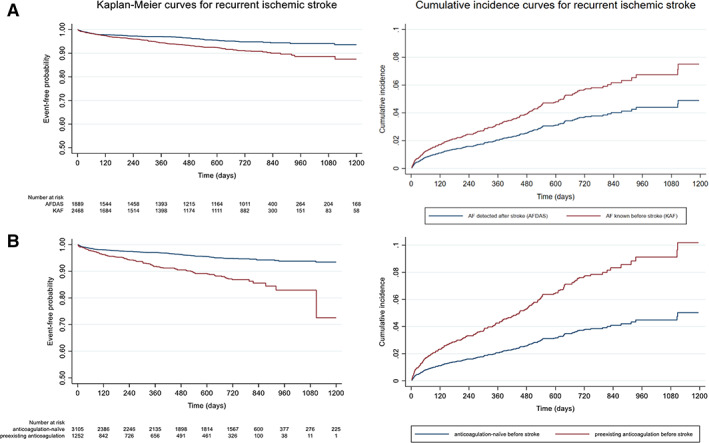
Of 4,357 patients, 1,889 (43%) had AFDAS and 2,468 (57%) had KAF, while 3,105 (71%) were anticoagulation-naïve before stroke and 1,252 (29%) were previously anticoagulated. During 6,071 patient-years of follow-up, we observed 244 recurrent strokes and 661 deaths. Only pre-existing anticoagulation (but not KAF) was independently associated with a higher hazard for stroke recurrence in both Cox and Fine-Gray models. Models incorporating pre-existing anticoagulation showed better fit than those with AF category; adding AF-category did not result in better model fit. Neither pre-existing anticoagulation nor KAF were independently associated with death.
Our findings challenge the notion that KAF and AFDAS are clinically relevant and distinct prognostic entities. Instead of attributing an independently high stroke recurrence risk to KAF, future research should focus on the causes of stroke despite anticoagulation to develop improved preventive treatments. ANN NEUROL 2023;94:43-54.
已知在缺血性卒中(KAF)之前发生的心房颤动(AF)被认为是一种独立的类别,其复发风险高于卒中后发现的心房颤动(AFDAS)。然而,尚不清楚这种风险差异是否因预先存在的抗凝治疗而混淆,这种治疗在 KAF 中最常见,也表明缺血性卒中复发风险较高。
对 5 个前瞻性抗凝治疗的 AF 相关缺血性卒中患者队列的个体患者数据进行分析。我们使用多变量 Cox、Fine-Gray 模型和拟合优度统计来比较 AFDAS 与 KAF 患者、抗凝治疗初治患者与既往抗凝治疗患者的主要(缺血性卒中复发)和次要结局(全因死亡),以调查 AF 类别和预先存在的抗凝治疗相对独立的预后重要性。
在 4357 例患者中,1889 例(43%)为 AFDAS,2468 例(57%)为 KAF,3105 例(71%)在卒中前未接受抗凝治疗,1252 例(29%)为既往抗凝治疗。在 6071 患者年的随访期间,我们观察到 244 例复发卒中,661 例死亡。只有预先存在的抗凝治疗(而非 KAF)与 Cox 和 Fine-Gray 模型中的卒中复发风险增加独立相关。包含预先存在的抗凝治疗的模型显示比包含 AF 类别的模型拟合更好;添加 AF 类别不会导致更好的模型拟合。预先存在的抗凝治疗和 KAF 均与死亡无关。
我们的研究结果挑战了 KAF 和 AFDAS 是临床相关和独特的预后实体的观点。未来的研究不应将 KAF 归因于独立的高卒中复发风险,而应关注尽管进行抗凝治疗但仍发生卒中的原因,以开发更好的预防治疗方法。ANN NEUROL 2023;94:43-54。