Diouf Adama, Adom Theodosia, Aouidet Abdel, El Hamdouchi Asmaa, Joonas Noorjehan I, Loechl Cornelia U, Leyna Germana H, Mbithe Dorcus, Moleah Thabisile, Monyeki Andries, Nashandi Hilde Liisa, Somda Serge Ma, Reilly John J
Laboratoire de Nutrition, Département de Biologie Animale, Faculté des Sciences et Techniques, Université Cheikh Anta Diop de Dakar, BP 5005 Dakar Fann, Senegal.
Nutrition Research Centre, Ghana Atomic Energy Commission, Accra, Ghana.
Bull World Health Organ. 2018 Nov 1;96(11):772-781. doi: 10.2471/BLT.17.205948. Epub 2018 Sep 10.
To compare the World Health Organization (WHO) body mass index (BMI)-for-age definition of obesity against measured body fatness in African children.
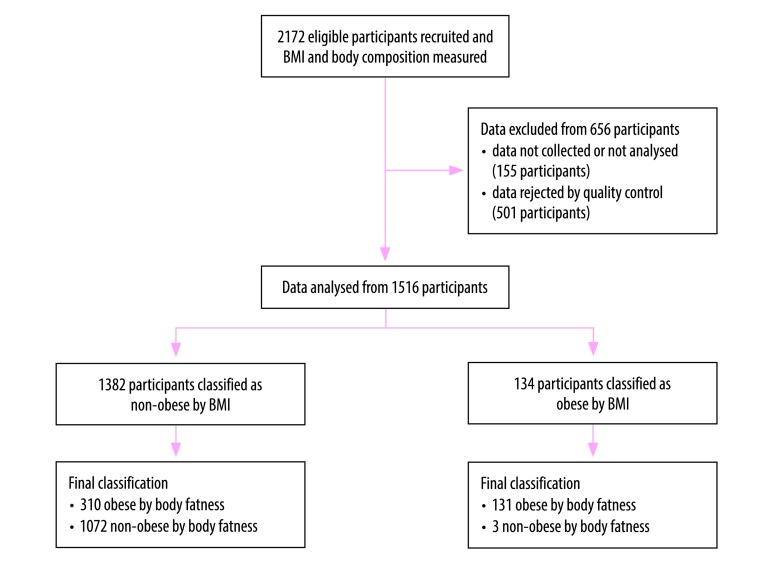
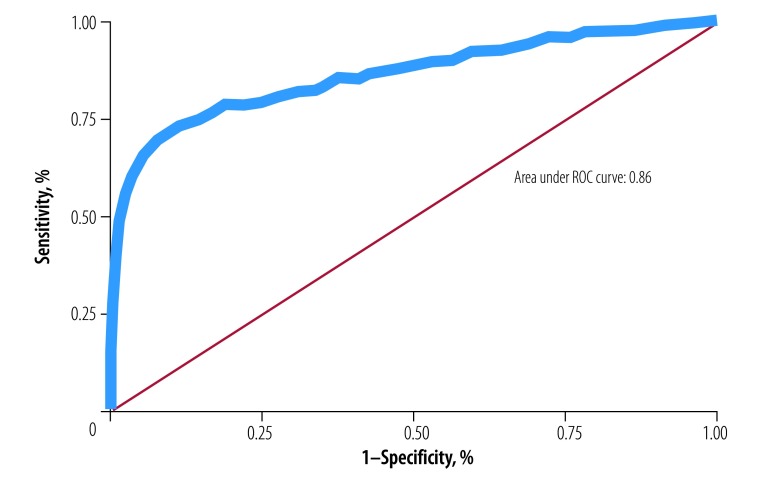
In a prospective multicentre study over 2013 to 2017, we recruited 1516 participants aged 8 to 11 years old from urban areas of eight countries (Ghana, Kenya, Mauritius, Morocco, Namibia, Senegal, Tunisia and United Republic of Tanzania). We measured height and weight and calculated BMI-for-age using WHO standards. We measured body fatness using the deuterium dilution method and defined excessive body fat percentage as > 25% in boys and > 30% in girls. We calculated the sensitivity and specificity of BMI z-score > +2.00 standard deviations (SD) and used receiver operating characteristic analysis and the Youden index to determine the optimal BMI z-score cut-off for classifying excessive fatness.
The prevalence of excessive fatness was over three times higher than BMI-for-age-defined obesity: 29.1% (95% CI: 26.8 to 31.4; 441 children) versus 8.8% (95% CI: 7.5 to 10.4; 134 children). The sensitivity of BMI z-score > +2.00 SD was low (29.7%, 95% CI: 25.5 to 34.2) and specificity was high (99.7%, 95% CI: 99.2 to 99.9). The receiver operating characteristic analysis found that a BMI z-score +0.58 SD would optimize sensitivity, and at this cut-off the area under the curve was 0.86, sensitivity 71.9% (95% CI: 67.4 to 76.0) and specificity 91.1% (95% CI: 89.2 to 92.7).
While BMI remains a practical tool for obesity surveillance, it underestimates excessive fatness and this should be considered when planning future African responses to the childhood obesity pandemic.
比较世界卫生组织(WHO)年龄别体重指数(BMI)对肥胖的定义与非洲儿童实测体脂情况。
在2013年至2017年的一项前瞻性多中心研究中,我们从八个国家(加纳、肯尼亚、毛里求斯、摩洛哥、纳米比亚、塞内加尔、突尼斯和坦桑尼亚联合共和国)的城市地区招募了1516名8至11岁的参与者。我们测量了身高和体重,并使用WHO标准计算年龄别BMI。我们使用氘稀释法测量体脂,并将男孩体脂百分比>25%和女孩体脂百分比>30%定义为体脂过多。我们计算了BMI z评分>+2.00标准差(SD)的敏感性和特异性,并使用受试者工作特征分析和尤登指数来确定用于分类体脂过多的最佳BMI z评分临界值。
体脂过多的患病率比年龄别BMI定义的肥胖高出三倍多:29.1%(95%CI:26.8至31.4;441名儿童),而年龄别BMI定义的肥胖为8.8%(95%CI:7.5至10.4;134名儿童)。BMI z评分>+2.00 SD的敏感性较低(29.7%,95%CI:25.5至34.2),特异性较高(99.7%,95%CI:99.2至99.9)。受试者工作特征分析发现,BMI z评分+0.58 SD可优化敏感性,在此临界值下,曲线下面积为0.86,敏感性为71.9%(95%CI:67.4至76.0),特异性为91.1%(95%CI:89.2至92.7)。
虽然BMI仍然是肥胖监测的实用工具,但它低估了体脂过多的情况,在规划未来非洲应对儿童肥胖流行的措施时应考虑到这一点。