Chong Shaur-Zheng, Fang Chih-Yuan, Fang Hsiu-Yu, Chen Huang-Chung, Chen Chien-Jen, Yang Cheng-Hsu, Hang Chi-Ling, Yip Hon-Kan, Wu Chiung-Jen, Lee Wei-Chieh
Division of Cardiology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung 833, Taiwan.
Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan 701, Taiwan.
J Clin Med. 2018 Nov 20;7(11):452. doi: 10.3390/jcm7110452.
Acute fulminant myocarditis (AFM) is a serious disease that progresses rapidly, and leads to failing respiratory and circulatory systems. When medications fail to reverse the patient's clinical course, extracorporeal membrane oxygenation (ECMO) is considered the most effective, supportive and adjunct strategy. In this paper we analyzed our experience in managing AFM with ECMO support.
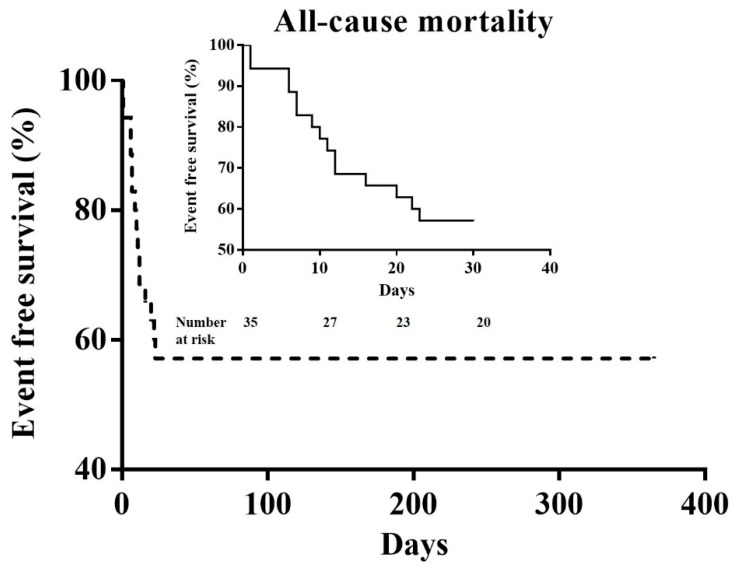
During October 2003 and February 2017, a total of 35 patients (≥18 years) were enrolled in the study. Twenty patients survived, and another 15 patients expired. General demographics, the hemodynamic condition, timing of ECMO intervention, and laboratory data were compared for the survival and non-survival groups. Univariate and multivariate Cox regression analyses were performed to identify the associations with in-hospital mortality following ECMO use in this situation.
The survival rate was 57.1% during the in-hospital period. The average age, gender, severity of the hemodynamic condition, and cardiac rhythm were similar between the survival and non-survival groups. Higher serum lactic acid (initial and 24 h later), higher peak cardiac biomarkers, higher incidence of acute kidney injury and the need for hemodialysis were noted in the non-survival group. Higher 24-h lactic acid levels and higher peak troponin-I levels were associated with in-hospital mortality.
When ECMO was used for AFM, related cardiogenic shock and decompensated heart failure, higher peak serum troponin-I levels and 24-h serum lactic acid levels following ECMO use were independently associated with in-hospital mortality.
急性暴发性心肌炎(AFM)是一种进展迅速的严重疾病,可导致呼吸和循环系统衰竭。当药物治疗无法逆转患者的临床病程时,体外膜肺氧合(ECMO)被认为是最有效、最具支持性的辅助策略。在本文中,我们分析了我们在ECMO支持下管理AFM的经验。
在2003年10月至2017年2月期间,共有35名年龄≥18岁的患者纳入本研究。20名患者存活,另外15名患者死亡。比较了存活组和非存活组的一般人口统计学资料、血流动力学状况、ECMO干预时机和实验室数据。进行单因素和多因素Cox回归分析,以确定在这种情况下使用ECMO后与院内死亡率的关联。
住院期间存活率为57.1%。存活组和非存活组之间的平均年龄、性别、血流动力学状况严重程度和心律相似。非存活组的血清乳酸水平(初始时和24小时后)更高、心脏生物标志物峰值更高、急性肾损伤发生率更高以及需要血液透析。24小时乳酸水平升高和肌钙蛋白-I峰值升高与院内死亡率相关。
当ECMO用于AFM时,相关的心源性休克和失代偿性心力衰竭、ECMO使用后血清肌钙蛋白-I峰值水平升高和24小时血清乳酸水平升高与院内死亡率独立相关。