Dave Bharat Rajendraprasad, Samal Puspak, Sangvi Romin, Degulmadi Devanand, Patel Denish, Krishnan Ajay
Department of Spine Surgery, Stavya Spine Hospital and Research Institute, Ahmedabad, India.
Asian Spine J. 2019 Apr;13(2):198-209. doi: 10.31616/asj.2018.0168. Epub 2018 Nov 27.
A retrospective comparative analysis of 64 patients with cauda equina syndrome (CES), who underwent either decompression alone (NF) or fusion (F) surgery.
We compared the outcomes and timing effects.
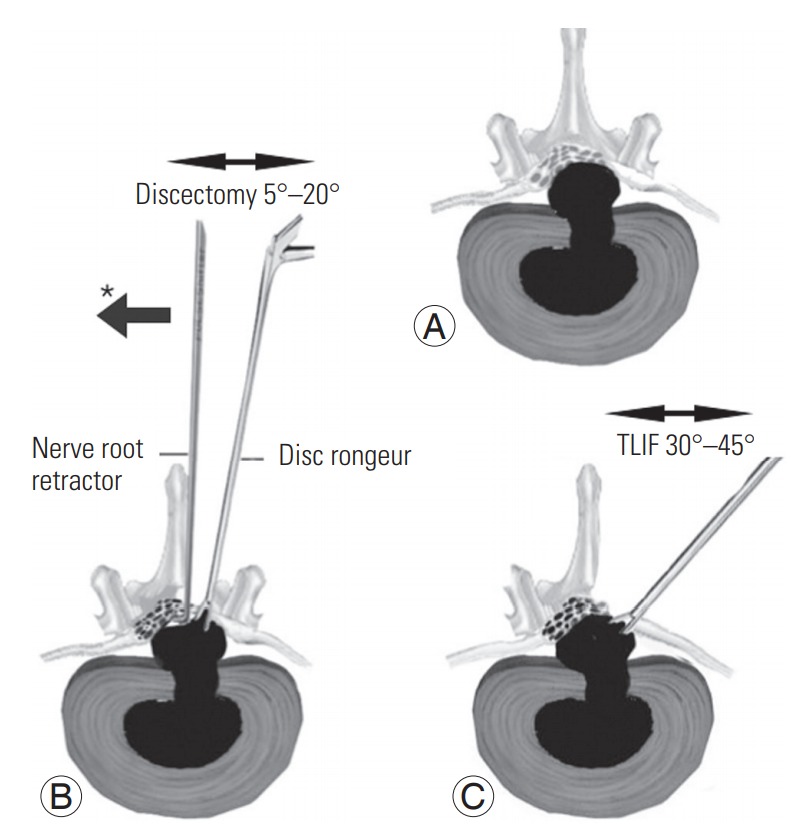
CES can cause loss of autonomic control of vesicular function and lower limb neurological deficits. Prompt diagnosis and emergency surgery markedly improve outcome. Although decompression only is a mainstream technique, there is guarded recovery of vesicular dysfunction. Decompression ventrally in a narrow window requires manipulation of neural tissue in an already jeopardised critical canal and may accentuate irreversible damages. In F surgery, the adequate exposure leads to a lower neural manipulation.
Until January 2008, we treated CES with decompression (laminectomy and/or discectomy). However, from that month forward, all our single-level CES patients have received a fusion operation. In this study, characteristic categorical variables and outcomes were analysed.
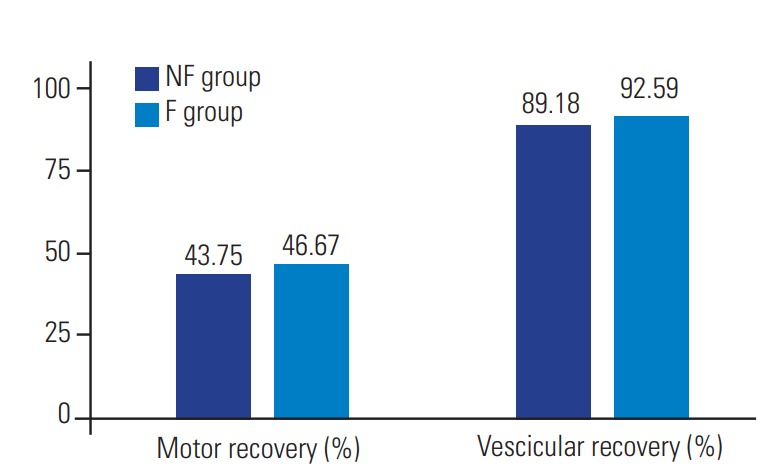
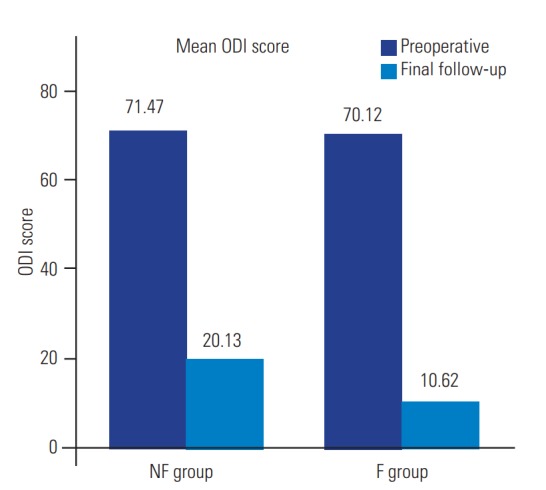
In a retrospective analysis of 64 patients, NF (n=37) and F (n=27) who received treatment, we found that both groups improved significantly on follow-up in all objective parameters. Although, the comparison of clinical and functional outcome data between the two groups was statistically insignificant, the average value of objective outcome such as vesicular function, low back pain (LBP), and complications was better for patients in F group compared with NF group. However, the patient satisfaction for the F group was also lower, in view of their residual symptoms and disabilities. Contrary to common perceptions, we found that the timing of surgery does not influence the recovery rate for either approach.
Although both the techniques appear to be equally effective, the fusion approach overall showed a definite edge over non-fusion, with respect to reduced incidence of iatrogenic dural tears, LBP, and overall outcome, even despite the lower patient satisfaction.
对64例马尾神经综合征(CES)患者进行回顾性比较分析,这些患者接受了单纯减压(NF)或融合(F)手术。
我们比较了手术效果和时间效应。
CES可导致膀胱功能自主控制丧失和下肢神经功能缺损。及时诊断和急诊手术可显著改善预后。虽然单纯减压是一种主流技术,但膀胱功能障碍的恢复情况并不乐观。在狭窄视野下进行腹侧减压需要在已经受损的关键椎管内操作神经组织,这可能会加重不可逆转的损伤。在融合手术中,充分的暴露可减少对神经的操作。
直到2008年1月,我们采用减压术(椎板切除术和/或椎间盘切除术)治疗CES。然而,从那个月起,我们所有的单节段CES患者都接受了融合手术。在本研究中,对特征性分类变量和手术效果进行了分析。
在对64例接受治疗的患者(NF组37例,F组27例)进行的回顾性分析中,我们发现两组在所有客观参数的随访中均有显著改善。虽然两组之间的临床和功能结果数据比较在统计学上无显著差异,但与NF组相比,F组患者在膀胱功能、腰痛(LBP)和并发症等客观结果的平均值方面更好。然而,考虑到F组患者的残余症状和残疾情况,其患者满意度也较低。与普遍看法相反,我们发现手术时机对两种手术方法的恢复率均无影响。
虽然两种技术似乎同样有效,但融合手术总体上在减少医源性硬脊膜撕裂、LBP的发生率和总体手术效果方面比非融合手术有明显优势,尽管患者满意度较低。