Unit of Internal Medicine and Hepatology, Department of Medicine, University Campus Bio-Medico, Rome 00128, Italy.
World J Gastroenterol. 2018 Nov 21;24(43):4835-4845. doi: 10.3748/wjg.v24.i43.4835.
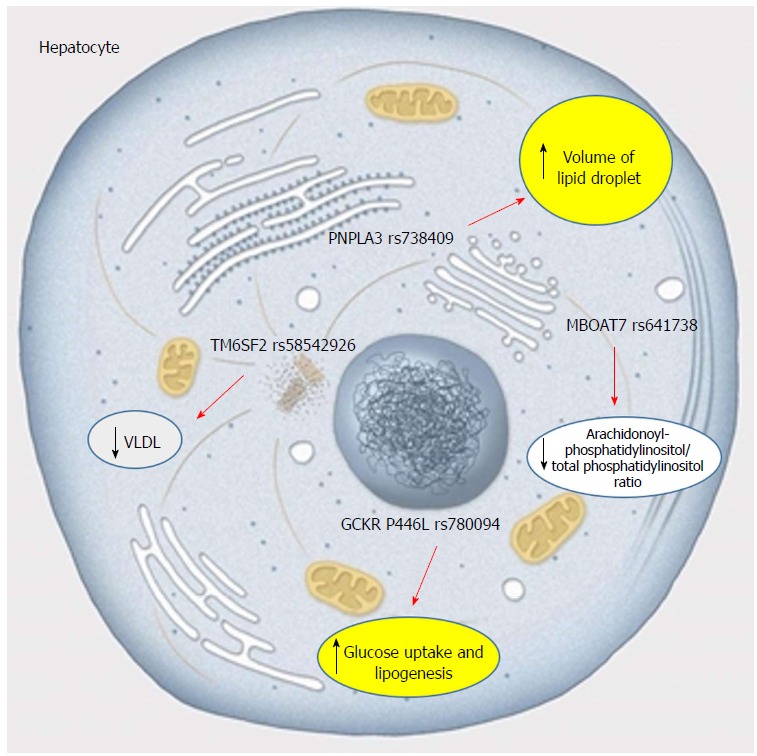
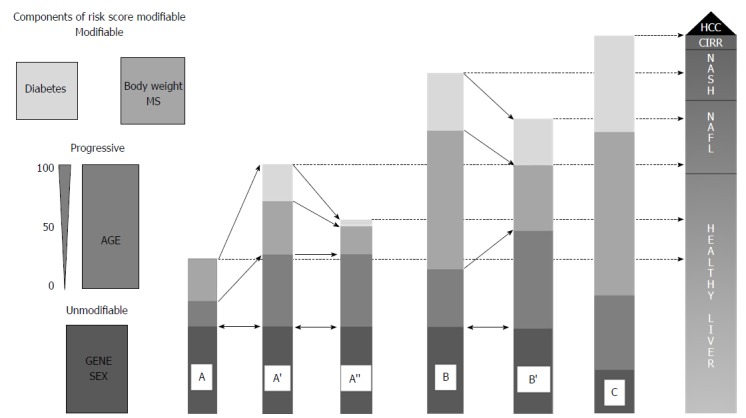
Non-alcoholic fatty liver disease (NAFLD) has a prevalence of approximately 30% in western countries, and is emerging as the first cause of liver cirrhosis and hepatocellular carcinoma (HCC). Therefore, risk stratification emerges as fundamental in order to optimize human and economic resources, and genetics displays intrinsic characteristics suitable to fulfill this task. According to the available data, heritability estimates for hepatic fat content range from 20% to 70%, and an almost 80% of shared heritability has been found between hepatic fat content and fibrosis. The rs738409 single nucleotide polymorphism (SNP) in patatin-like phospholipase domain-containing protein 3 gene and the rs58542926 SNP in transmembrane 6 superfamily member 2 gene have been robustly associated with NAFLD and with its progression, but promising results have been obtained with many other SNPs. Moreover, there has been proof of the additive role of the different SNPs in determining liver damage, and there have been preliminary experiences in which risk scores created through a few genetic variants, alone or in combination with clinical variables, were associated with a strongly potentiated risk of NAFLD, non-alcoholic steatohepatitis (NASH), NASH fibrosis or NAFLD-HCC. However, to date, clinical translation of genetics in the field of NAFLD has been poor or absent. Fortunately, the research we have done seems to have placed us on the right path: We should rely on longitudinal rather than on cross-sectional studies; we should focus on relevant outcomes rather than on simple liver fat accumulation; and we should put together the genetic and clinical information. The hope is that combined genetic/clinical scores, derived from longitudinal studies and built on a few strong genetic variants and relevant clinical variables, will reach a significant predictive power, such as to have clinical utility for risk stratification at the single patient level and even to esteem the impact of intervention on the risk of disease-related outcomes. Well-structured future studies would demonstrate if this vision can become a reality.
非酒精性脂肪性肝病(NAFLD)在西方国家的患病率约为 30%,正在成为肝硬化和肝细胞癌(HCC)的首要原因。因此,风险分层对于优化人力和经济资源至关重要,而遗传学具有内在的特征,适合完成这项任务。根据现有数据,肝脂肪含量的遗传力估计范围为 20%至 70%,并且在肝脂肪含量和纤维化之间发现了近 80%的共享遗传力。载脂蛋白样磷脂酶结构域包含蛋白 3 基因中的 rs738409 单核苷酸多态性(SNP)和跨膜 6 超家族成员 2 基因中的 rs58542926 SNP 与 NAFLD 及其进展密切相关,但许多其他 SNP 也取得了有希望的结果。此外,已经证明不同 SNP 在确定肝损伤方面具有累加作用,并且已经有初步经验表明,通过少数遗传变异单独或与临床变量结合创建的风险评分与 NAFLD、非酒精性脂肪性肝炎(NASH)、NASH 纤维化或 NAFLD-HCC 的风险呈强烈增强相关。然而,迄今为止,NAFLD 领域的遗传学临床转化一直很差或不存在。幸运的是,我们所做的研究似乎使我们走上了正确的道路:我们应该依赖于纵向研究而不是横断面研究;我们应该关注相关的结果而不是简单的肝脂肪堆积;我们应该将遗传和临床信息结合起来。希望基于纵向研究并基于少数强遗传变异和相关临床变量构建的联合遗传/临床评分能够具有显著的预测能力,例如能够在个体患者水平上进行风险分层,甚至可以评估干预对疾病相关结果风险的影响。未来结构良好的研究将证明这一愿景是否能够成为现实。