Department of Cardiovascular Sciences, University of Leicester and Cardiovascular Theme, NIHR Leicester Biomedical Research Centre, Glenfield Hospital, Groby road, Leicester, LE3 9QP, UK.
Xinapse Systems Ltd., West Bergholt, Essex, CO6 3BW, UK.
Eur Radiol. 2019 May;29(5):2340-2349. doi: 10.1007/s00330-018-5775-6. Epub 2018 Nov 28.
To compare aortic size and stiffness parameters on MRI between bicuspid aortic valve (BAV) and tricuspid aortic valve (TAV) patients with aortic stenosis (AS).
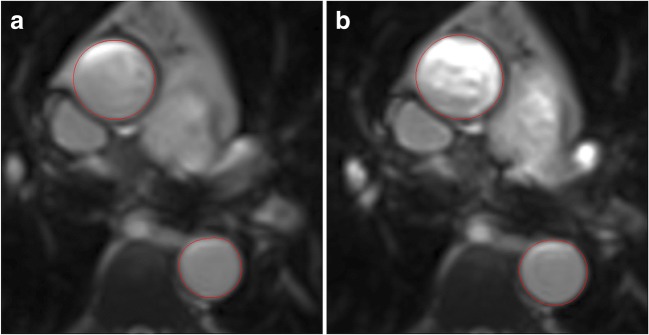
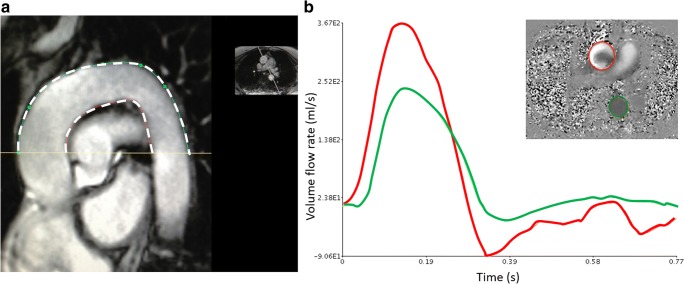
MRI was performed in 174 patients with asymptomatic moderate-severe AS (mean AVAI 0.57 ± 0.14 cm/m) and 23 controls on 3T scanners. Valve morphology was available/analysable in 169 patients: 63 BAV (41 type-I, 22 type-II) and 106 TAV. Aortic cross-sectional areas were measured at the level of the pulmonary artery bifurcation. The ascending and descending aorta (AA, DA) distensibility, and pulse wave velocity (PWV) around the aortic arch were calculated.
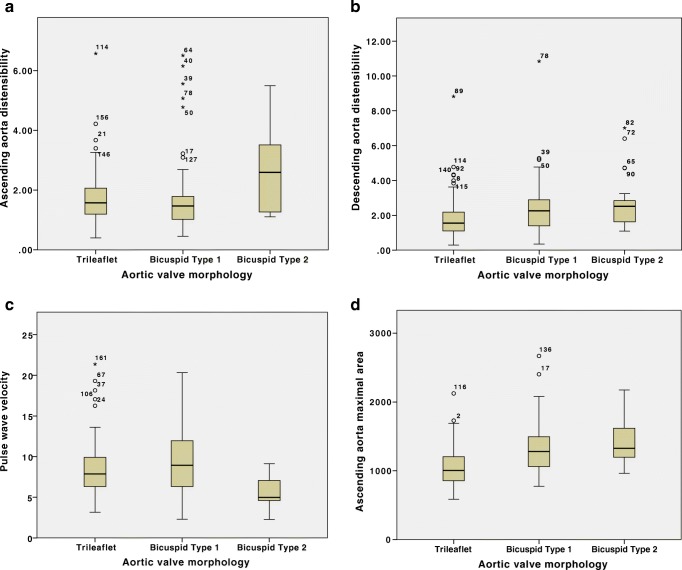
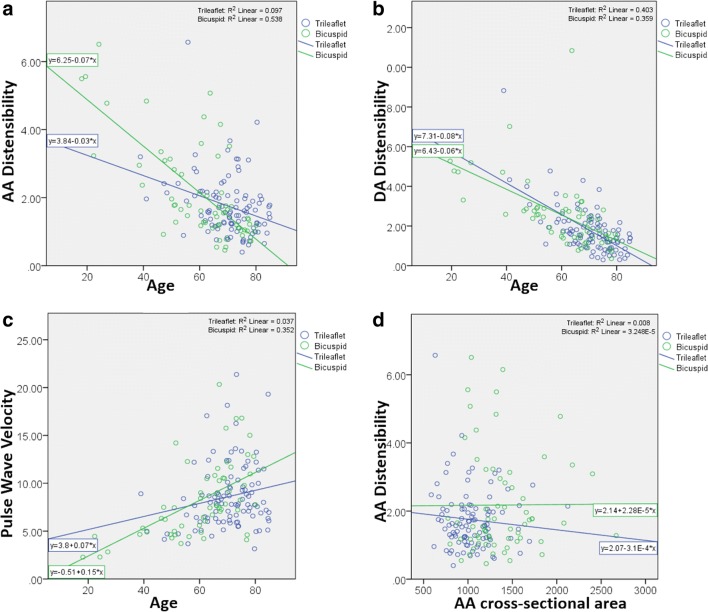
The AA and DA areas were lower in the controls, with no difference in DA distensibility or PWV, but slightly lower AA distensibility than in the patient group. With increasing age, there was a decrease in distensibility and an increase in PWV. After correcting for age, the AA maximum cross-sectional area was higher in bicuspid vs. tricuspid patients (12.97 [11.10, 15.59] vs. 10.06 [8.57, 12.04] cm, p < 0.001), but there were no significant differences in AA distensibility (p = 0.099), DA distensibility (p = 0.498) or PWV (p = 0.235). Patients with BAV type-II valves demonstrated a significantly higher AA distensibility and lower PWV compared to type-I, despite a trend towards higher AA area.
In patients with significant AS, BAV patients do not have increased aortic stiffness compared to those with TAV despite increased ascending aortic dimensions. Those with type-II BAV have less aortic stiffness despite greater dimensions. These results demonstrate a dissociation between aortic dilatation and stiffness and suggest that altered flow patterns may play a role.
• Both cellular abnormalities secondary to genetic differences and abnormal flow patterns have been implicated in the pathophysiology of aortic dilatation and increased vascular complications associated with bicuspid aortic valves (BAV). • We demonstrate an increased ascending aortic size in patients with BAV and moderate to severe AS compared to TAV and controls, but no difference in aortic stiffness parameters, therefore suggesting a dissociation between dilatation and stiffness. • Sub-group analysis showed greater aortic size but lower stiffness parameters in those with BAV type-II AS compared to BAV type-I.
比较 MRI 显示的二叶式主动脉瓣(BAV)和三叶式主动脉瓣(TAV)主动脉瓣狭窄(AS)患者的主动脉大小和僵硬度参数。
在 3T 扫描仪上对 174 例无症状中重度 AS(平均 AVAI 0.57±0.14 cm/m)患者和 23 例对照者进行 MRI 检查。在 169 例患者中可获得/可分析瓣膜形态:63 例 BAV(41 例 I 型,22 例 II 型)和 106 例 TAV。在肺动脉分叉处测量主动脉的横截面积。计算升主动脉(AA)和降主动脉(DA)的可扩展性以及主动脉弓周围的脉搏波速度(PWV)。
对照组的 AA 和 DA 面积较低,DA 扩展性或 PWV 无差异,但 AA 扩展性略低于患者组。随着年龄的增长,可扩展性降低,PWV 增加。校正年龄后,二叶瓣患者的 AA 最大横截面积高于三叶瓣患者(12.97[11.10,15.59] vs. 10.06[8.57,12.04] cm,p<0.001),但 AA 扩展性(p=0.099)、DA 扩展性(p=0.498)或 PWV(p=0.235)无显著差异。与 I 型相比,II 型 BAV 患者的 AA 扩展性更高,PWV 更低,尽管 AA 面积有增大趋势。
在有明显 AS 的患者中,与 TAV 患者相比,BAV 患者的主动脉僵硬度没有增加,尽管升主动脉尺寸增大。尽管二叶瓣患者的升主动脉尺寸较大,但主动脉僵硬度较低。这些结果表明主动脉扩张和僵硬度之间存在分离,并提示血流模式的改变可能起作用。
细胞异常继发于遗传差异和异常的血流模式,与二叶式主动脉瓣(BAV)相关的主动脉扩张和增加的血管并发症的病理生理学有关。
我们发现,与 TAV 和对照组相比,二叶瓣主动脉瓣狭窄(AS)患者的升主动脉尺寸增大,但主动脉僵硬度参数无差异,因此提示扩张和僵硬度之间存在分离。
亚组分析显示,与二叶瓣 I 型相比,二叶瓣 II 型 AS 患者的主动脉尺寸更大,但僵硬度参数更低。