Downey Candice, Randell Rebecca, Brown Julia, Jayne David G
Leeds Institute of Biomedical & Clinical Sciences, University of Leeds, Leeds, United Kingdom.
School of Healthcare, University of Leeds, Leeds, United Kingdom.
J Med Internet Res. 2018 Dec 11;20(12):e10802. doi: 10.2196/10802.
Vital signs monitoring is a universal tool for the detection of postoperative complications; however, unwell patients can be missed between traditional observation rounds. New remote monitoring technologies promise to convey the benefits of continuous monitoring to patients in general wards.
The aim of this pilot study was to evaluate whether continuous remote vital signs monitoring is a practical and acceptable way of monitoring surgical patients and to optimize the delivery of a definitive trial.
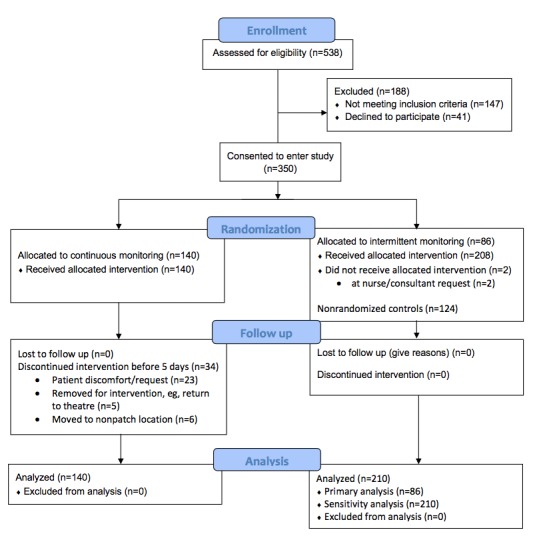
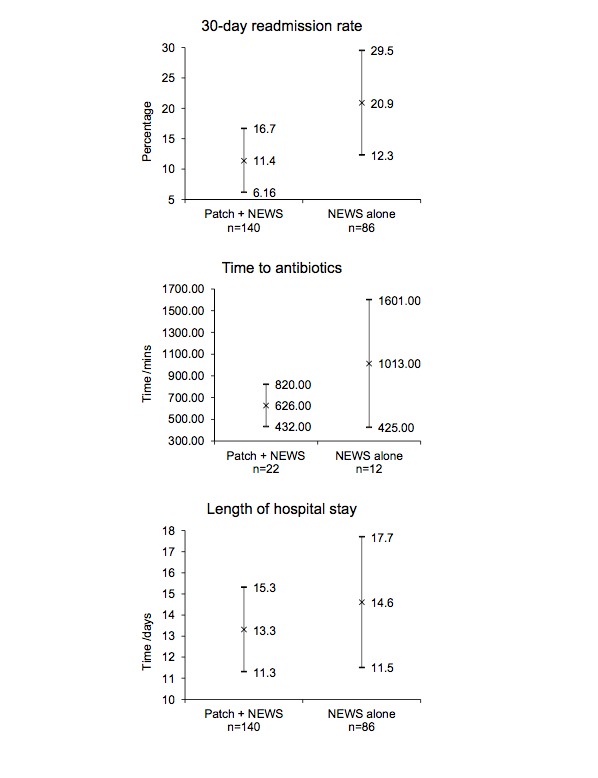
We performed a prospective, cluster-randomized, parallel-group, unblinded, controlled pilot study. Patients admitted to 2 surgical wards at a large tertiary hospital received either continuous and intermittent vital signs monitoring or intermittent monitoring alone using an early warning score system. Continuous monitoring was provided by a wireless patch, worn on the patient's chest, with data transmitted wirelessly every 2 minutes to a central monitoring station or a mobile device carried by the patient's nurse. The primary outcome measure was time to administration of antibiotics in sepsis. The secondary outcome measures included the length of hospital stay, 30-day readmission rate, mortality, and patient acceptability.
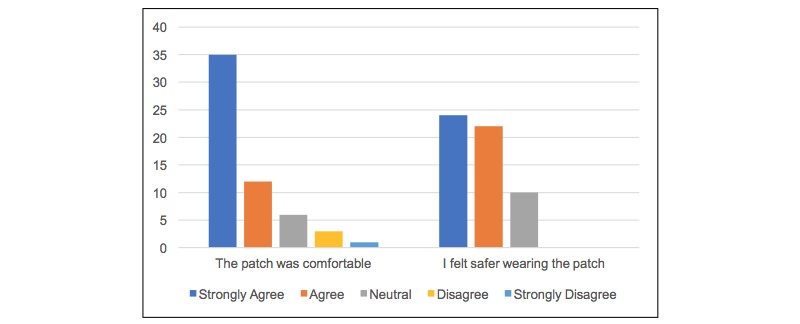
Overall, 226 patients were randomized between January and June 2017. Of 226 patients, 140 were randomized to continuous remote monitoring and 86 to intermittent monitoring alone. On average, patients receiving continuous monitoring were administered antibiotics faster after evidence of sepsis (626 minutes, n=22, 95% CI 431.7-820.3 minutes vs 1012.8 minutes, n=12, 95% CI 425.0-1600.6 minutes), had a shorter average length of hospital stay (13.3 days, 95% CI 11.3-15.3 days vs 14.6 days, 95% CI 11.5-17.7 days), and were less likely to require readmission within 30 days of discharge (11.4%, 95% CI 6.16-16.7 vs 20.9%, 95% CI 12.3-29.5). Wide CIs suggest these differences are not statistically significant. Patients found the monitoring device to be acceptable in terms of comfort and perceived an enhanced sense of safety, despite 24% discontinuing the intervention early.
Remote continuous vital signs monitoring on surgical wards is practical and acceptable to patients. Large, well-controlled studies in high-risk populations are required to determine whether the observed trends translate into a significant benefit for continuous over intermittent monitoring.
International Standard Randomised Controlled Trial Number ISRCTN60999823; http://www.isrctn.com /ISRCTN60999823 (Archived by WebCite at http://www.webcitation.org/73ikP6OQz).

生命体征监测是检测术后并发症的通用工具;然而,在传统的观察轮次之间,不适的患者可能会被遗漏。新的远程监测技术有望将持续监测的益处带给普通病房的患者。
这项试点研究的目的是评估持续远程生命体征监测是否是监测手术患者的一种实用且可接受的方式,并优化确定性试验的实施。
我们进行了一项前瞻性、整群随机、平行组、非盲、对照试点研究。在一家大型三级医院的2个外科病房住院的患者,使用早期预警评分系统,要么接受持续和间歇性生命体征监测,要么仅接受间歇性监测。持续监测由佩戴在患者胸部的无线贴片提供,数据每2分钟无线传输到中央监测站或患者护士携带的移动设备。主要结局指标是脓毒症中抗生素给药时间。次要结局指标包括住院时间、30天再入院率、死亡率和患者可接受性。
总体而言,2017年1月至6月期间有226名患者被随机分组。在226名患者中,140名被随机分配到持续远程监测组,86名被随机分配到仅间歇性监测组。平均而言,有脓毒症证据后,接受持续监测的患者抗生素给药更快(626分钟,n = 22,95%CI 431.7 - 820.3分钟,相比1012.8分钟,n = 12,95%CI 425.0 - 1600.6分钟),平均住院时间更短(13.3天,95%CI 11.3 - 15.3天,相比14.6天,95%CI 11.5 - 17.7天),并且在出院后30天内再次入院的可能性更小(11.4%,95%CI 6.16 - 16.7,相比20.9%,95%CI 12.3 - 29.5)。宽置信区间表明这些差异无统计学意义。患者认为监测设备在舒适度方面是可接受的,并且感觉安全感增强,尽管24%的患者提前终止了干预。
外科病房的远程持续生命体征监测对患者来说是实用且可接受的。需要在高危人群中进行大型、严格控制的研究,以确定观察到的趋势是否转化为持续监测相对于间歇性监测的显著益处。
国际标准随机对照试验编号ISRCTN60999823;http://www.isrctn.com /ISRCTN60999823(由WebCite存档于http://www.webcitation.org/73ikP6OQz)