Nephrology Section, Department of Internal Medicine, Ghent University Hospital, Ghent, Belgium; and.
National Health and Medical Research Council Clinical Trials Centre, Sydney Medical School, University of Sydney, New South Wales, Australia.
Clin J Am Soc Nephrol. 2019 Jan 7;14(1):84-93. doi: 10.2215/CJN.08150718. Epub 2018 Dec 13.
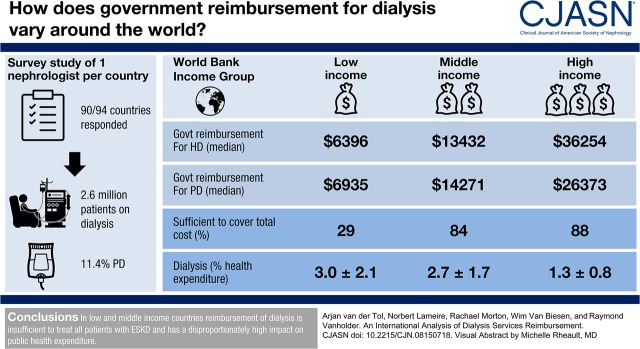
The prevalence of patients with ESKD who receive extracorporeal kidney replacement therapy is rising worldwide. We compared government reimbursement for hemodialysis and peritoneal dialysis worldwide, assessed the effect on the government health care budget, and discussed strategies to reduce the cost of kidney replacement therapy.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: Cross-sectional global survey of nephrologists in 90 countries to assess reimbursement for dialysis, number of patients receiving hemodialysis and peritoneal dialysis, and measures to prevent development or progression of CKD, conducted online July to December of 2016.
Of the 90 survey respondents, governments from 81 countries (90%) provided reimbursement for maintenance dialysis. The prevalence of patients per million population being treated with long-term dialysis in low- and middle-income countries increased linearly with Gross Domestic Product per capita (GDP per capita), but was substantially lower in these countries compared with high-income countries where we did not observe an higher prevalence with higher GDP per capita. The absolute expenditure for dialysis by national governments showed a positive association with GDP per capita, but the percent of total health care budget spent on dialysis showed a negative association. The percentage of patients on peritoneal dialysis was low, even in countries where peritoneal dialysis is better reimbursed than hemodialysis. The so-called peritoneal dialysis-first policy without financial incentive seems to be effective in increasing the utilization of peritoneal dialysis. Few countries actively provide CKD prevention.
In low- and middle-income countries, reimbursement of dialysis is insufficient to treat all patients with ESKD and has a disproportionately high effect on public health expenditure. Current reimbursement policies favor conventional in-center hemodialysis.
全球范围内,接受体外肾脏替代疗法的终末期肾病(ESKD)患者的患病率正在上升。我们比较了全球范围内血液透析和腹膜透析的政府报销情况,评估了对政府医疗保健预算的影响,并讨论了降低肾脏替代治疗成本的策略。
设计、设置、参与者和测量:2016 年 7 月至 12 月,对 90 个国家的 90 名肾病学家进行了一项横断面全球调查,以评估透析的报销情况、接受血液透析和腹膜透析的患者人数,以及预防慢性肾脏病(CKD)发展或进展的措施。
在 90 名调查对象中,81 个国家(90%)的政府提供维持性透析的报销。中低收入国家每百万人口接受长期透析治疗的患者患病率与人均国内生产总值(人均 GDP)呈线性相关,但与高收入国家相比,这些国家的患病率明显较低,而高收入国家的人均 GDP 并未导致更高的患病率。各国政府对透析的绝对支出与人均 GDP 呈正相关,但用于透析的总医疗保健预算的百分比与人均 GDP 呈负相关。腹膜透析的比例较低,即使在腹膜透析报销优于血液透析的国家也是如此。没有经济激励的所谓腹膜透析优先政策似乎可以有效地增加腹膜透析的利用率。很少有国家积极提供 CKD 预防措施。
在中低收入国家,透析的报销不足以治疗所有的终末期肾病患者,对公共卫生支出的影响不成比例地高。现行的报销政策有利于传统的中心血液透析。