Cancer Prevention Program, Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, Washington, USA.
Department of Epidemiology, University of Washington, Seattle, Washington, USA.
Compr Physiol. 2018 Dec 13;9(1):1-58. doi: 10.1002/cphy.c170040.
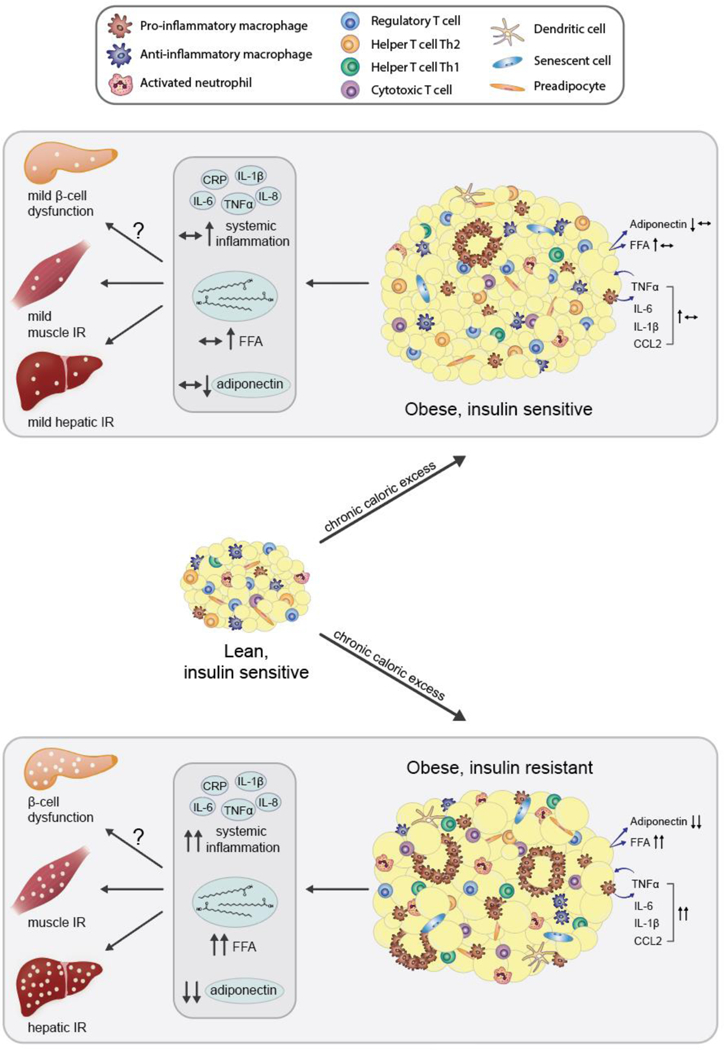
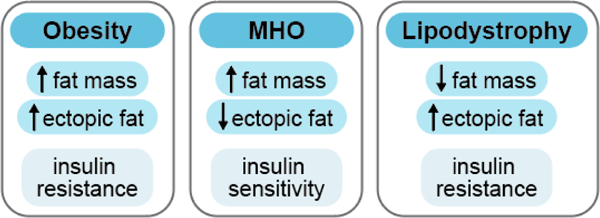
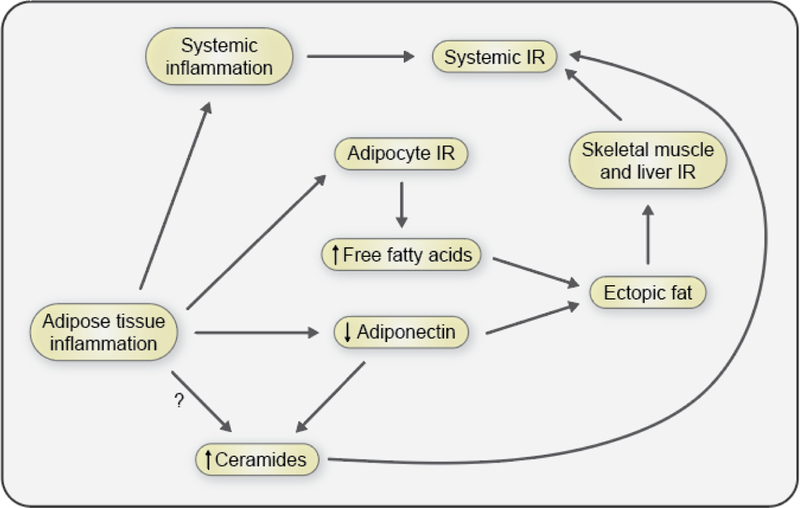
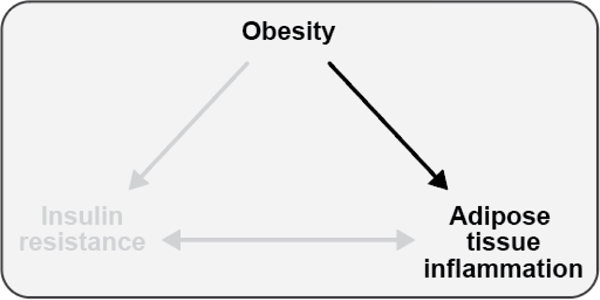
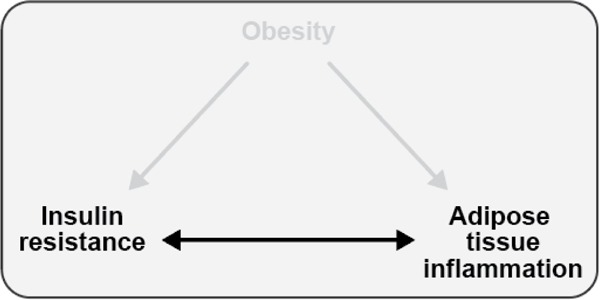
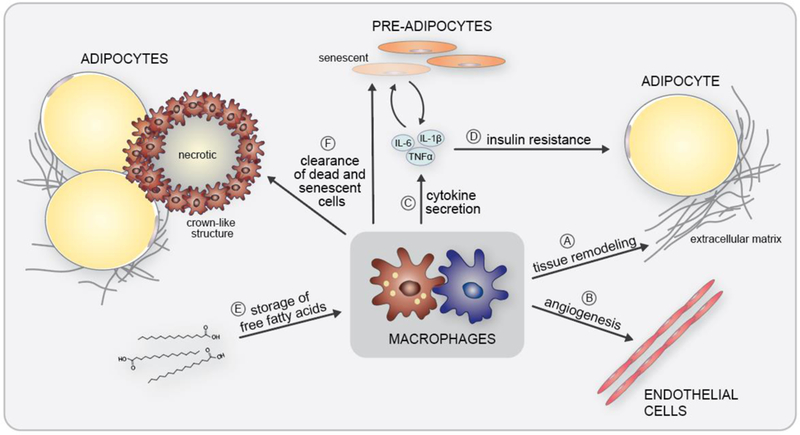
The objective of this comprehensive review is to summarize and discuss the available evidence of how adipose tissue inflammation affects insulin sensitivity and glucose tolerance. Low-grade, chronic adipose tissue inflammation is characterized by infiltration of macrophages and other immune cell populations into adipose tissue, and a shift toward more proinflammatory subtypes of leukocytes. The infiltration of proinflammatory cells in adipose tissue is associated with an increased production of key chemokines such as C-C motif chemokine ligand 2, proinflammatory cytokines including tumor necrosis factor α and interleukins 1β and 6 as well as reduced expression of the key insulin-sensitizing adipokine, adiponectin. In both rodent models and humans, adipose tissue inflammation is consistently associated with excess fat mass and insulin resistance. In humans, associations with insulin resistance are stronger and more consistent for inflammation in visceral as opposed to subcutaneous fat. Further, genetic alterations in mouse models of obesity that reduce adipose tissue inflammation are-almost without exception-associated with improved insulin sensitivity. However, a dissociation between adipose tissue inflammation and insulin resistance can be observed in very few rodent models of obesity as well as in humans following bariatric surgery- or low-calorie-diet-induced weight loss, illustrating that the etiology of insulin resistance is multifactorial. Taken together, adipose tissue inflammation is a key factor in the development of insulin resistance and type 2 diabetes in obesity, along with other factors that likely include inflammation and fat accumulation in other metabolically active tissues. © 2019 American Physiological Society. Compr Physiol 9:1-58, 2019.
本综述的目的是总结和讨论脂肪组织炎症如何影响胰岛素敏感性和葡萄糖耐量的现有证据。低度、慢性脂肪组织炎症的特征是巨噬细胞和其他免疫细胞群浸润脂肪组织,以及白细胞向更具炎症性的亚型转变。促炎细胞在脂肪组织中的浸润与关键趋化因子(如 C-C 基序趋化因子配体 2)、炎症细胞因子(包括肿瘤坏死因子-α和白细胞介素 1β和 6)的产生增加以及关键胰岛素增敏脂肪因子脂联素的表达减少有关。在啮齿动物模型和人类中,脂肪组织炎症与脂肪量过多和胰岛素抵抗一致相关。在人类中,与胰岛素抵抗的相关性对于内脏脂肪而非皮下脂肪的炎症更强且更一致。此外,肥胖小鼠模型中减少脂肪组织炎症的遗传改变几乎无一例外地与胰岛素敏感性的改善相关。然而,在极少数肥胖的啮齿动物模型以及减肥手术后或低热量饮食引起的体重减轻的人类中,可以观察到脂肪组织炎症和胰岛素抵抗之间的分离,这表明胰岛素抵抗的病因是多因素的。总之,脂肪组织炎症是肥胖中胰岛素抵抗和 2 型糖尿病发展的关键因素,其他可能包括其他代谢活跃组织中的炎症和脂肪堆积等因素也起作用。 美国生理学学会。综合生理学 9:1-58, 2019.