Kim Bun, Kim Byung Chang, Kim Jeongseon, Oh Hyun Jin, Ryu Kum Hei, Park Bum Joon, Sohn Dae Kyung, Hong Chang Won, Han Kyung Su
Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
Center for Cancer Prevention and Detection, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
Yonsei Med J. 2019 Jan;60(1):73-78. doi: 10.3349/ymj.2019.60.1.73.
Prior abdomino-pelvic (AP) surgery makes colonoscopy difficult and can affect bowel preparation quality. However, bowel preparation quality has been found to vary according to prior AP surgery type. We examined the relationship of prior AP surgery type with bowel preparation quality in a large-scale retrospective cohort.
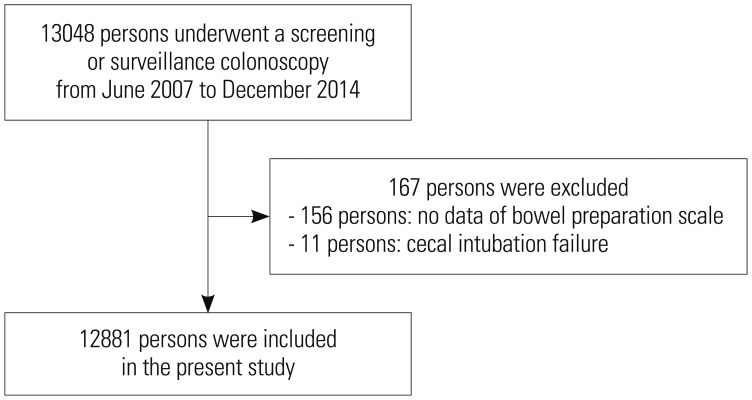
In the health screening cohort of the National Cancer Center, 12881 participants who underwent screening or surveillance colonoscopy between June 2007 and December 2014 were included. Personal data were collected by reviewing patient medical records. Bowel preparation quality was assessed using the Aronchick scale and was categorized as satisfactory for excellent to good bowel preparation or unsatisfactory for fair to inadequate bowel preparation.
A total of 1557 (12.1%) participants had a history of AP surgery. The surgery types were colorectal surgery (n=44), gastric/small intestinal surgery (n=125), appendectomy/peritoneum/laparotomy (n=476), cesarean section (n=278), uterus/ovarian surgery (n=317), kidney/bladder/prostate surgery (n=19), or liver/pancreatobiliary surgery (n=96). The proportion of satisfactory bowel preparations was 70.7%. In multivariate analysis, unsatisfactory bowel preparation was related to gastric/small intestinal surgery (odds ratio=1.764, 95% confidence interval=1.230-2.532, =0.002). However, the other surgery types did not affect bowel preparation quality. Current smoking, diabetes, and high body mass index were risk factors of unacceptable bowel preparation.
Only gastric/small intestinal surgery was a potential risk factor for poor bowel preparation. Further research on patients with a history of gastric/small intestinal surgery to determine appropriate methods for adequate bowel preparation is mandatory.
既往腹盆腔(AP)手术会使结肠镜检查变得困难,并可能影响肠道准备质量。然而,已发现肠道准备质量会因既往AP手术类型的不同而有所差异。我们在一个大规模回顾性队列中研究了既往AP手术类型与肠道准备质量之间的关系。
纳入国家癌症中心健康筛查队列中在2007年6月至2014年12月期间接受筛查或监测结肠镜检查的12881名参与者。通过查阅患者病历收集个人数据。使用阿隆奇克量表评估肠道准备质量,并将其分类为肠道准备良好至优秀为满意,肠道准备一般至不足为不满意。
共有1557名(12.1%)参与者有AP手术史。手术类型包括结直肠手术(n = 44)、胃/小肠手术(n = 125)、阑尾切除术/腹膜/剖腹术(n = 476)、剖宫产(n = 278)、子宫/卵巢手术(n = 317)、肾脏/膀胱/前列腺手术(n = 19)或肝脏/胰胆手术(n = 96)。满意的肠道准备比例为70.7%。在多变量分析中,不满意的肠道准备与胃/小肠手术相关(比值比 = 1.764,95%置信区间 = 1.230 - 2.532,P = 0.002)。然而,其他手术类型并不影响肠道准备质量。当前吸烟、糖尿病和高体重指数是肠道准备不合格的危险因素。
只有胃/小肠手术是肠道准备不佳的潜在危险因素。必须对有胃/小肠手术史的患者进行进一步研究,以确定适当的充分肠道准备方法。