Department of Thoracic and Cardiovascular Surgery, Cleveland Clinic, Cleveland, Ohio; Department of Quantitative Health Sciences, Cleveland Clinic, Cleveland, Ohio.
Department of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai, New York, NY.
J Thorac Cardiovasc Surg. 2019 Jan;157(1):234-243.e9. doi: 10.1016/j.jtcvs.2018.06.093. Epub 2018 Jul 27.
To use novel statistical methods for analyzing the effect of lesion set on (long-standing) persistent atrial fibrillation (AF) in the Cardiothoracic Surgical Trials Network trial of surgical ablation during mitral valve surgery (MVS).
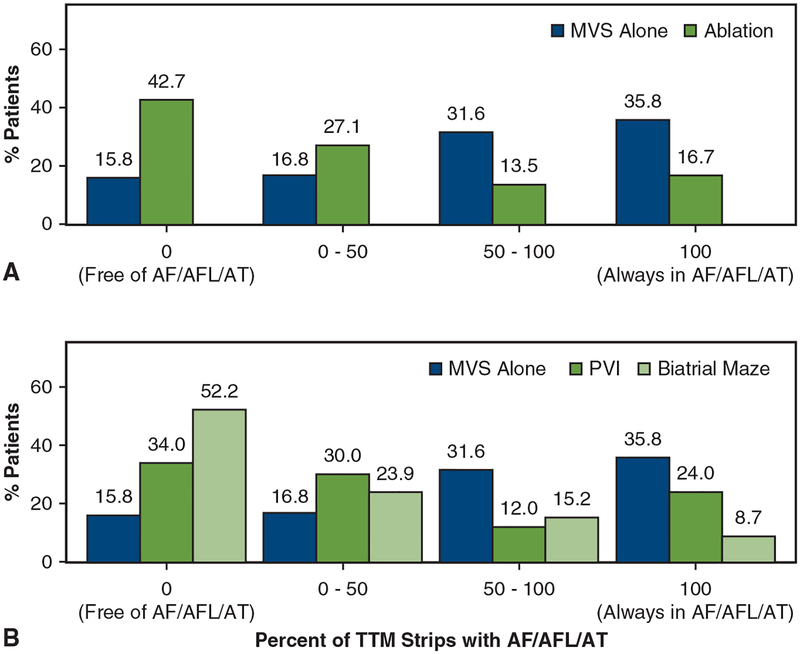
Two hundred sixty such patients were randomized to MVS + surgical ablation or MVS alone. Ablation was randomized between pulmonary vein isolation and biatrial maze. During 12 months postsurgery, 228 patients (88%) submitted 7949 transtelephonic monitoring (TTM) recordings, analyzed for AF, atrial flutter (AFL), or atrial tachycardia (AT). As previously reported, more ablation than MVS-alone patients were free of AF or AF/AFL at 6 and 12 months (63% vs 29%; P < .001) by 72-hour Holter monitoring, without evident difference between lesion sets (for which the trial was underpowered).
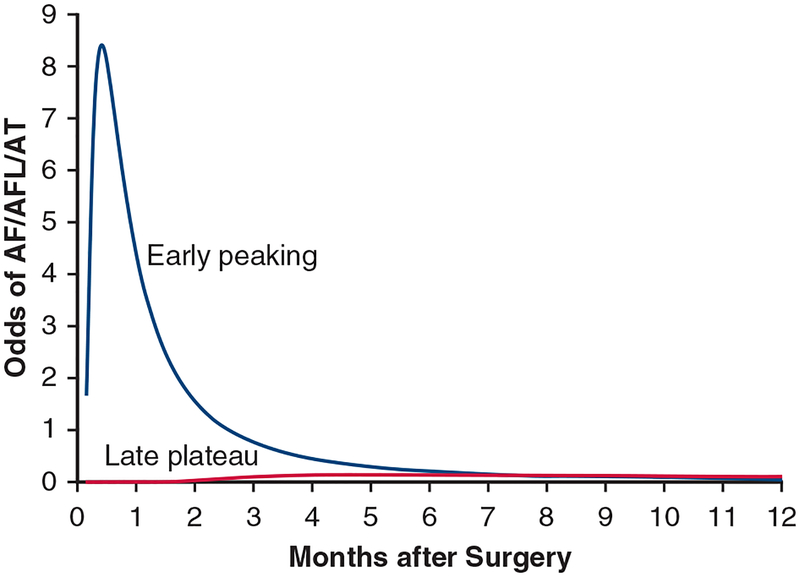
Estimated freedom from AF/AFL/AT on any transmission trended higher after biatrial maze than pulmonary vein isolation (odds ratio, 2.31; 95% confidence interval, 0.95-5.65; P = .07) 3 to 12 months postsurgery; estimated AF/AFL/AT load (ie, proportion of TTM strips recording AF/AFL/AT) was similar (odds ratio, 0.90; 95% confidence interval, 0.57-1.43; P = .6). Within 12 months, estimated prevalence of AF/AFL/AT by TTM was 58% after MVS alone, and 36% versus 23% after pulmonary vein isolation versus biatrial maze (P < .02).
Statistical modeling using TTM recordings after MVS in patients with (long-standing) persistent AF suggests that a biatrial maze is associated with lower AF/AFL/AT prevalence, but not a lower load, compared with pulmonary vein isolation. The discrepancy between AF/AFL/AT prevalence assessed at 2 time points by Holter monitoring versus weekly TTM suggests the need for a confirmatory trial, reassessment of definitions for failure after ablation, and validation of statistical methods for assessing atrial rhythms longitudinally.
使用新的统计方法分析心脏外科学临床试验网络二尖瓣手术(MVS)期间手术消融治疗(持续性)长期持续性心房颤动(AF)的病变组对(持续性)长期持续性 AF 的影响。
260 例患者随机分为 MVS+手术消融组或 MVS 组。消融在肺静脉隔离和双房迷宫之间随机进行。术后 12 个月,228 例患者(88%)提交了 7949 次远程电话监测(TTM)记录,分析 AF、心房扑动(AFL)或房性心动过速(AT)。如前所述,通过 72 小时 Holter 监测,与 MVS 单一组相比,更多的消融患者在 6 个月和 12 个月时无 AF 或 AF/AFL(63% vs. 29%;P<.001),两组之间的病变组无明显差异(该试验没有足够的效力)。
在术后 3 至 12 个月,双房迷宫后 AF/AFL/AT 无心律失常的可能性高于肺静脉隔离(优势比,2.31;95%置信区间,0.95-5.65;P=0.07);AF/AFL/AT 负荷(即 TTM 记录 AF/AFL/AT 的比例)相似(优势比,0.90;95%置信区间,0.57-1.43;P=0.6)。在 12 个月内,MVS 单一组的 TTM 估计 AF/AFL/AT 发生率为 58%,肺静脉隔离组和双房迷宫组分别为 36%和 23%(P<.02)。
在 MVS 后使用 TTM 记录对(持续性)长期持续性 AF 患者进行统计建模表明,与肺静脉隔离相比,双房迷宫与较低的 AF/AFL/AT 发生率相关,但与较低的负荷无关。Holter 监测和每周 TTM 评估的 2 个时间点的 AF/AFL/AT 发生率之间的差异表明,需要进行验证性试验、消融后失败的定义重新评估,以及对纵向评估心房节律的统计方法进行验证。