Norfolk and Norwich University Hospital, Norwich, United Kingdom.
Academic Department of Medical Genetics, Addenbrooke's Hospital, University of Cambridge, Cambridge, United Kingdom.
Hepatology. 2019 May;69(5):2120-2135. doi: 10.1002/hep.30479. Epub 2019 Mar 4.
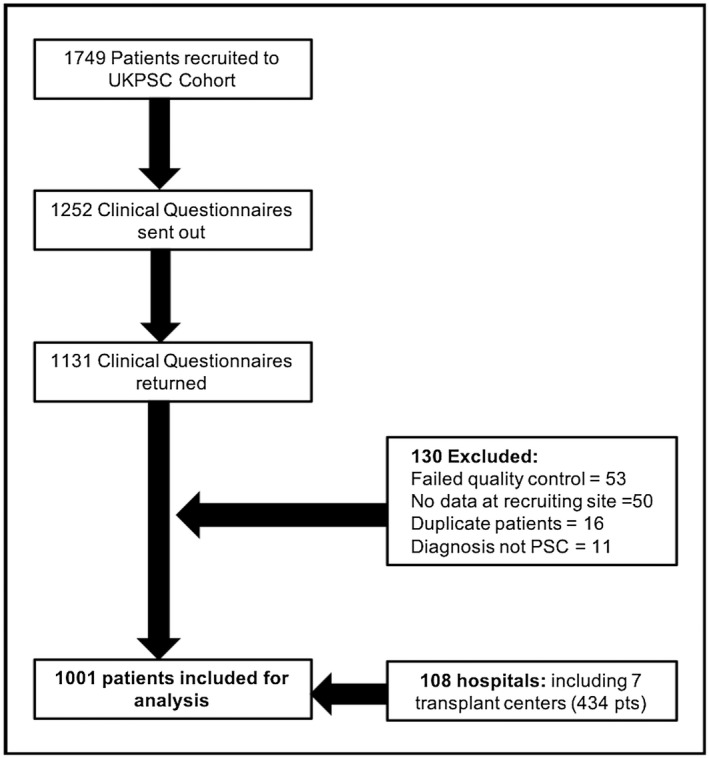
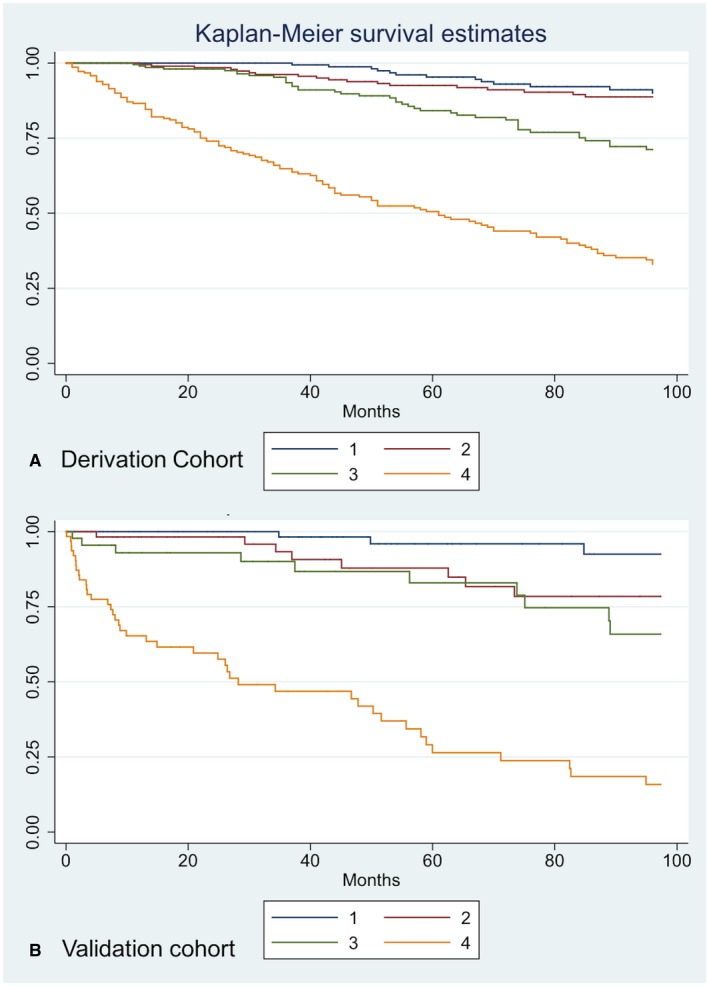
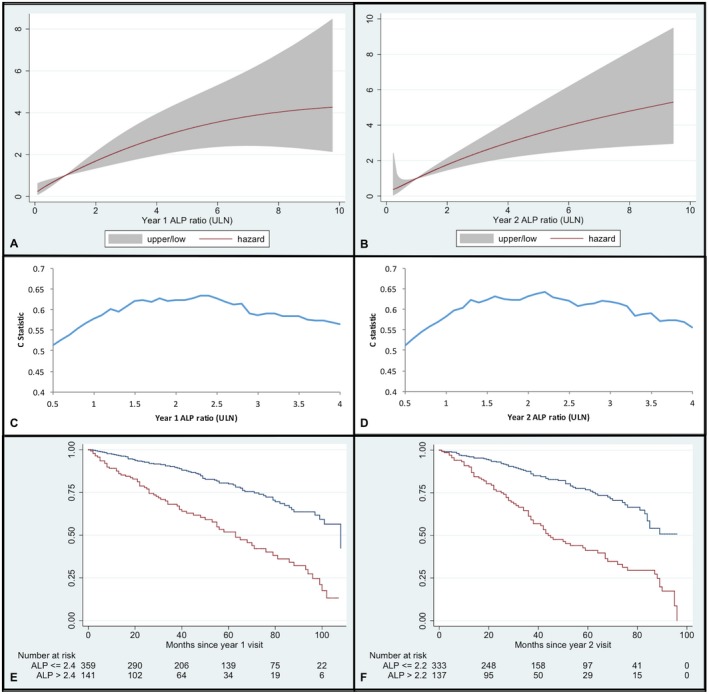
We sought to identify factors that are predictive of liver transplantation or death in patients with primary sclerosing cholangitis (PSC), and to develop and validate a contemporaneous risk score for use in a real-world clinical setting. Analyzing data from 1,001 patients recruited to the UK-PSC research cohort, we evaluated clinical variables for their association with 2-year and 10-year outcome through Cox-proportional hazards and C-statistic analyses. We generated risk scores for short-term and long-term outcome prediction, validating their use in two independent cohorts totaling 451 patients. Thirty-six percent of the derivation cohort were transplanted or died over a cumulative follow-up of 7,904 years. Serum alkaline phosphatase of at least 2.4 × upper limit of normal at 1 year after diagnosis was predictive of 10-year outcome (hazard ratio [HR] = 3.05; C = 0.63; median transplant-free survival 63 versus 108 months; P < 0.0001), as was the presence of extrahepatic biliary disease (HR = 1.45; P = 0.01). We developed two risk scoring systems based on age, values of bilirubin, alkaline phosphatase, albumin, platelets, presence of extrahepatic biliary disease, and variceal hemorrhage, which predicted 2-year and 10-year outcomes with good discrimination (C statistic = 0.81 and 0.80, respectively). Both UK-PSC risk scores were well-validated in our external cohort and outperformed the Mayo Clinic and aspartate aminotransferase-to-platelet ratio index (APRI) scores (C statistic = 0.75 and 0.63, respectively). Although heterozygosity for the previously validated human leukocyte antigen (HLA)-DR*03:01 risk allele predicted increased risk of adverse outcome (HR = 1.33; P = 0.001), its addition did not improve the predictive accuracy of the UK-PSC risk scores. Conclusion: Our analyses, based on a detailed clinical evaluation of a large representative cohort of participants with PSC, furthers our understanding of clinical risk markers and reports the development and validation of a real-world scoring system to identify those patients most likely to die or require liver transplantation.
我们旨在确定原发性硬化性胆管炎(PSC)患者肝移植或死亡的预测因素,并制定和验证适用于真实临床环境的同期风险评分。通过 Cox 比例风险和 C 统计分析,我们对来自英国 PSC 研究队列的 1001 名患者的数据进行了分析,评估了临床变量与 2 年和 10 年结局的相关性。我们生成了短期和长期结局预测的风险评分,并在两个共 451 名患者的独立队列中验证了其用途。在 7904 年的累积随访中,有 36%的队列在诊断后 1 年内接受了肝移植或死亡。诊断后 1 年内血清碱性磷酸酶(ALP)至少为正常值上限的 2.4 倍,提示 10 年结局(风险比[HR] = 3.05;C = 0.63;中位无移植生存 63 个月与 108 个月;P < 0.0001),肝外胆管疾病的存在也是如此(HR = 1.45;P = 0.01)。我们基于年龄、胆红素、ALP、白蛋白、血小板、肝外胆管疾病和静脉曲张出血的数值,制定了两个风险评分系统,可准确预测 2 年和 10 年的结局(C 统计值分别为 0.81 和 0.80)。两个英国 PSC 风险评分在我们的外部队列中得到了很好的验证,优于 Mayo 诊所和天门冬氨酸氨基转移酶与血小板比值指数(APRI)评分(C 统计值分别为 0.75 和 0.63)。虽然先前验证的人类白细胞抗原(HLA)-DR*03:01 风险等位基因的杂合性预示着不良结局的风险增加(HR = 1.33;P = 0.001),但其添加并未提高英国 PSC 风险评分的预测准确性。结论:我们的分析基于对大量代表性 PSC 患者进行详细的临床评估,进一步了解了临床风险标志物,并报告了真实世界评分系统的开发和验证,以确定最有可能死亡或需要肝移植的患者。