School of Public Health, IRSPUM, Université de Montréal, Montréal, Québec, H3N1X9, Canada.
School of Public Health, Université de Montréal, Montréal, Québec, Canada.
BMC Public Health. 2018 Dec 20;18(1):1398. doi: 10.1186/s12889-018-6261-4.
Primary care physicians (PCPs) working in mental health care in Tunisia often lack knowledge and skills needed to adequately address mental health-related issues. To address these lacunas, a training based on the Mental Health Gap Action Programme (mhGAP) Intervention Guide (IG) was offered to PCPs working in the Greater Tunis area between February and April 2016. While the mhGAP-IG has been used extensively in low- and middle-income countries (LMICs) to help build non-specialists' mental health capacity, little research has focused on how contextual factors interact with the implemented training program to influence its expected outcomes. This paper's objective is to fill that lack.
We conducted a case study with a purposeful sample of 18 trained PCPs. Data was collected by semi-structured interviews between March and April 2016. Qualitative data was analyzed using thematic analysis.
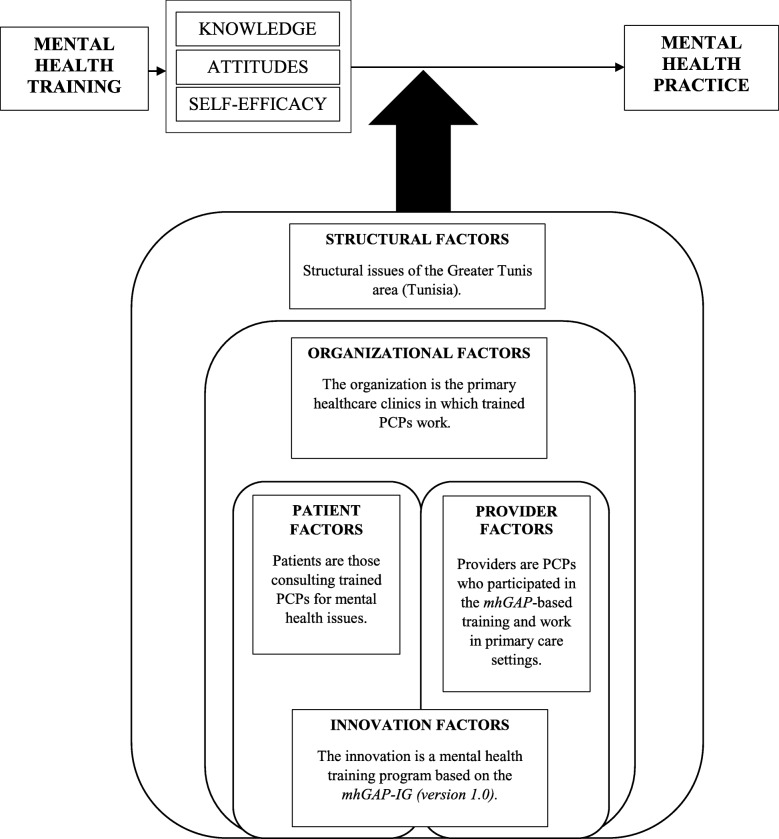
Participants identified more barriers than facilitators when describing contextual factors influencing the mhGAP-based training's expected outcomes. Barriers were regrouped into five categories: structural factors (e.g., policies, social context, local workforce development, and physical aspects of the environment), organizational factors (e.g., logistical issues for the provision of care and collaboration within and across healthcare organizations), provider factors (e.g., previous mental health experience and personal characteristics), patient factors (e.g., beliefs about the health system and healthcare professionals, and motivation to seek care), and innovation factors (e.g., training characteristics). These contextual factors interacted with the implemented training to influence knowledge about pharmacological treatments and symptoms of mental illness, confidence in providing treatment, negative beliefs about certain mental health conditions, and the understanding of the role of PCPs in mental health care delivery. In addition, post-training, participants still felt uncomfortable with certain aspects of treatment and the management of some mental health conditions.
Findings highlight the complexity of implementing a mhGAP-based training given its interaction with contextual factors to influence the attainment of expected outcomes. Results may be used to tailor structural, organizational, provider, patient, and innovation factors prior to future implementations of the mhGAP-based training in Tunisia. Findings may also be used by decision-makers interested in implementing the mhGAP-IG training in other LMICs.
在突尼斯,从事精神卫生保健工作的初级保健医生(PCP)往往缺乏充分解决与精神卫生相关问题所需的知识和技能。为了解决这些空白,2016 年 2 月至 4 月期间,在大突尼斯地区为从事精神卫生保健工作的 PCP 提供了一项基于《精神卫生差距行动规划(mhGAP)干预指南》(IG)的培训。虽然 mhGAP-IG 已在中低收入国家(LMICs)广泛用于帮助建立非专业人员的精神卫生能力,但很少有研究关注情境因素如何与实施的培训计划相互作用,从而影响预期结果。本文旨在填补这一空白。
我们对 18 名经过培训的 PCP 进行了一项案例研究,采用了有针对性的样本。数据收集于 2016 年 3 月至 4 月期间进行的半结构化访谈。使用主题分析对定性数据进行分析。
参与者在描述影响基于 mhGAP 的培训预期结果的情境因素时,认为障碍多于促进因素。障碍分为五类:结构性因素(例如,政策、社会背景、当地劳动力发展和环境的物质方面)、组织性因素(例如,提供护理的后勤问题以及医疗机构内部和跨医疗机构的合作)、提供者因素(例如,先前的精神卫生经验和个人特征)、患者因素(例如,对卫生系统和卫生保健专业人员的信念以及寻求护理的动机)和创新性因素(例如,培训特点)。这些情境因素与实施的培训相互作用,影响了对药物治疗和精神疾病症状的了解、提供治疗的信心、对某些精神卫生状况的负面看法以及对 PCP 在精神卫生保健提供中的作用的理解。此外,培训后,参与者对某些治疗方面和某些精神卫生状况的管理仍感到不适。
研究结果强调了实施基于 mhGAP 的培训的复杂性,因为其与情境因素相互作用,影响预期结果的实现。研究结果可用于突尼斯未来实施基于 mhGAP 的培训之前,对结构性、组织性、提供者、患者和创新性因素进行调整。对在其他 LMICs 实施 mhGAP-IG 培训感兴趣的决策者也可以使用这些结果。