Di Leo Angelo, O'Shaughnessy Joyce, Sledge George W, Martin Miguel, Lin Yong, Frenzel Martin, Hardebeck Molly C, Smith Ian C, Llombart-Cussac Antonio, Goetz Matthew P, Johnston Stephen
1Hospital of Prato, Istituto Toscano Tumori, Prato, Italy.
2Baylor University Medical Center, Texas Oncology, US Oncology, Dallas, TX USA.
NPJ Breast Cancer. 2018 Dec 18;4:41. doi: 10.1038/s41523-018-0094-2. eCollection 2018.
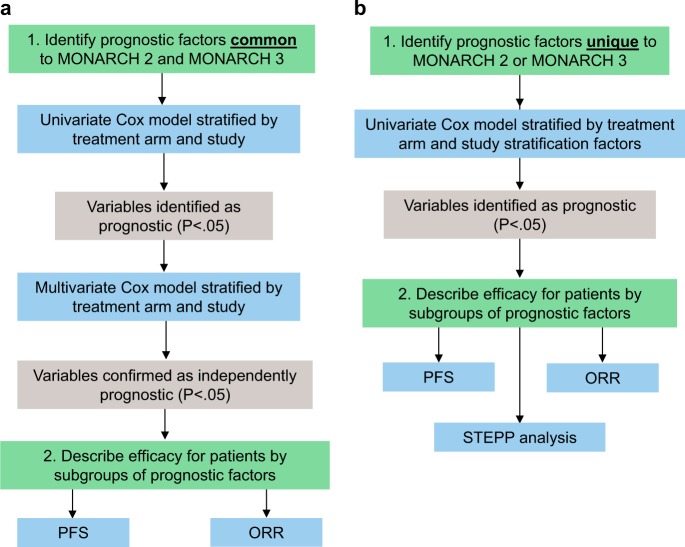
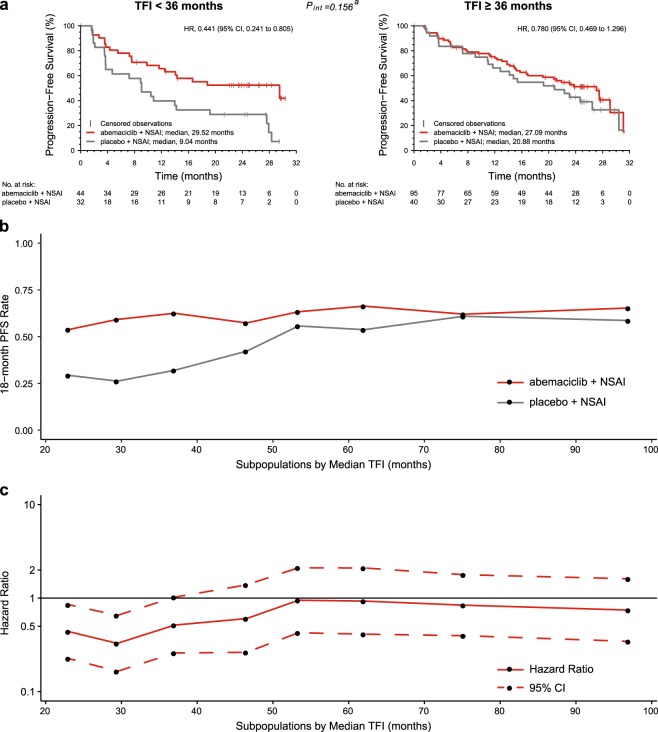
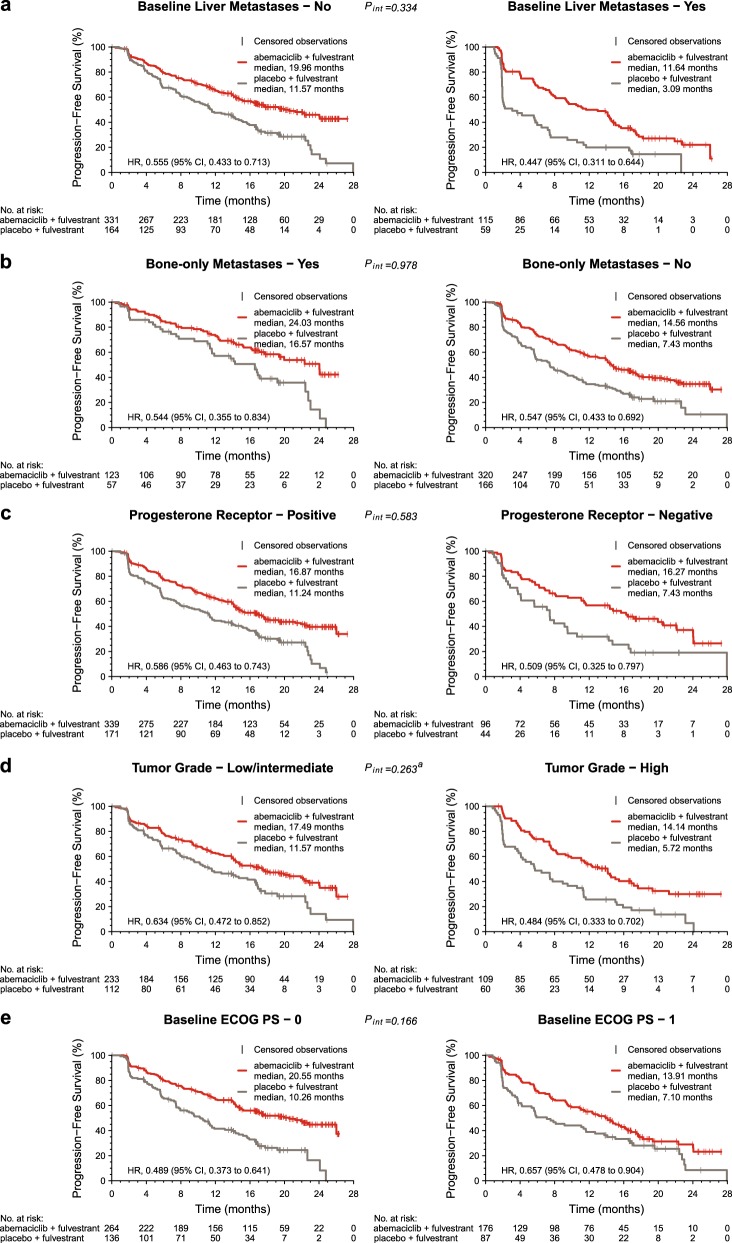
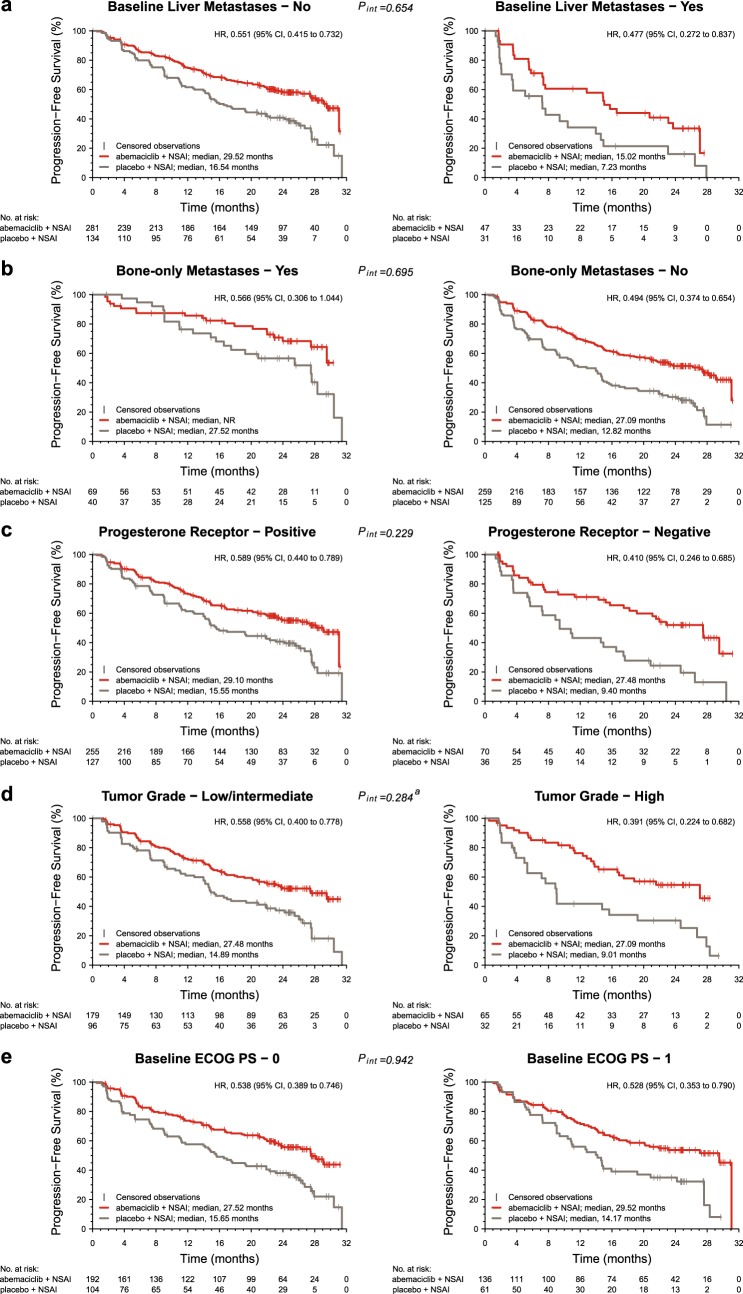
CDK4 & 6 inhibitors have enhanced the effectiveness of endocrine therapy (ET) in patients with advanced breast cancer (ABC). This paper presents exploratory analyses examining patient and disease characteristics that may inform in whom and when abemaciclib should be initiated. MONARCH 2 and 3 enrolled women with HR+, HER2- ABC. In MONARCH 2, patients whose disease had progressed while receiving ET were administered fulvestrant+abemaciclib/placebo. In MONARCH 3, patients received a nonsteroidal aromatase inhibitor+abemaciclib/placebo as initial therapy for advanced disease. A combined analysis of the two studies was performed to determine significant prognostic factors. Efficacy results (PFS and ORR in patients with measurable disease) were examined for patient subgroups corresponding to each significant prognostic factor. Analysis of clinical factors confirmed the following to have prognostic value: bone-only disease, liver metastases, tumor grade, progesterone receptor status, performance status, treatment-free interval (TFI) from the end of adjuvant ET, and time from diagnosis to recurrence. Prognosis was poorer in patients with liver metastases, progesterone receptor-negative tumors, high grade tumors, or short TFI (<36 months). Benefit (PFS hazard ratio, ORR increase) from abemaciclib was observed in all patient subgroups. Patients with indicators of poor prognosis had the largest benefit from the addition of abemaciclib. However, in MONARCH 3, for patients with certain good prognostic factors (TFI ≥ 36 months, bone-only disease) ET achieved a median PFS of >20 months. These analyses identified prognostic factors and demonstrated that patients with poor prognostic factors derived the largest benefit from the addition of abemaciclib.
细胞周期蛋白依赖性激酶4和6(CDK4 & 6)抑制剂提高了晚期乳腺癌(ABC)患者内分泌治疗(ET)的疗效。本文进行了探索性分析,以研究可能有助于确定阿贝西利应在何时、针对哪些患者开始使用的患者和疾病特征。MONARCH 2和3试验纳入了激素受体阳性(HR+)、人表皮生长因子受体2阴性(HER2-)的ABC女性患者。在MONARCH 2试验中,疾病在接受ET期间进展的患者接受氟维司群+阿贝西利/安慰剂治疗。在MONARCH 3试验中,患者接受非甾体芳香化酶抑制剂+阿贝西利/安慰剂作为晚期疾病的初始治疗。对这两项研究进行了联合分析,以确定显著的预后因素。针对与每个显著预后因素对应的患者亚组,检查了疗效结果(可测量疾病患者的无进展生存期和客观缓解率)。临床因素分析证实以下因素具有预后价值:仅骨转移疾病、肝转移、肿瘤分级、孕激素受体状态、体能状态、辅助内分泌治疗结束后的无治疗间期(TFI)以及从诊断到复发的时间。肝转移患者、孕激素受体阴性肿瘤患者、高级别肿瘤患者或TFI短(<36个月)的患者预后较差。在所有患者亚组中均观察到阿贝西利带来的获益(无进展生存期风险比、客观缓解率提高)。预后不良指标的患者从添加阿贝西利中获益最大。然而,在MONARCH 3试验中,对于某些具有良好预后因素(TFI≥36个月、仅骨转移疾病)的患者,内分泌治疗的中位无进展生存期>20个月。这些分析确定了预后因素,并表明预后不良因素的患者从添加阿贝西利中获益最大。