Department of Radiology, The Saban Research Institute, Children's Hospital Los Angeles, Los Angeles, California, United states of America.
Department of Pathology, Children's Hospital Los Angeles and Keck School of Medicine, University of Southern California, Los Angeles, California, United states of America.
PLoS One. 2019 Jan 4;14(1):e0206394. doi: 10.1371/journal.pone.0206394. eCollection 2019.
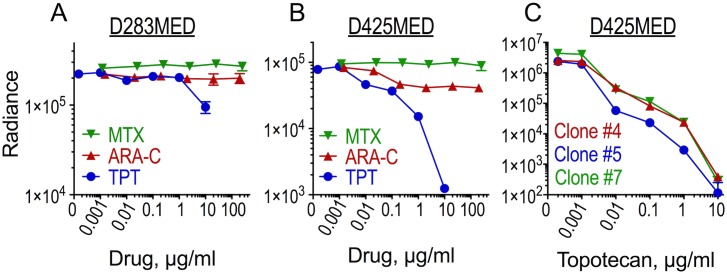
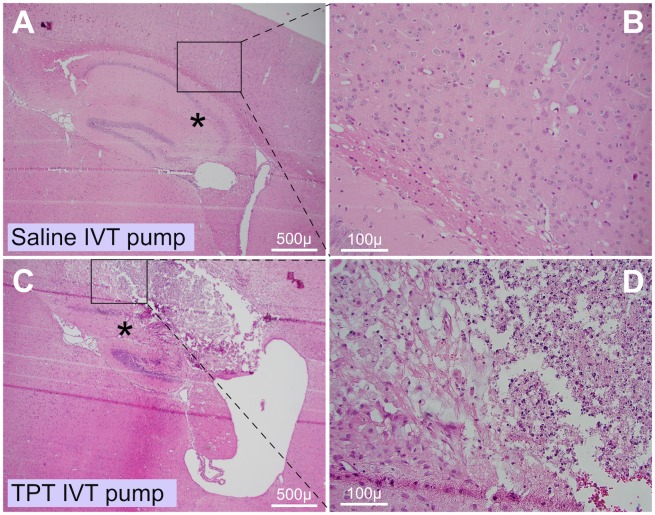
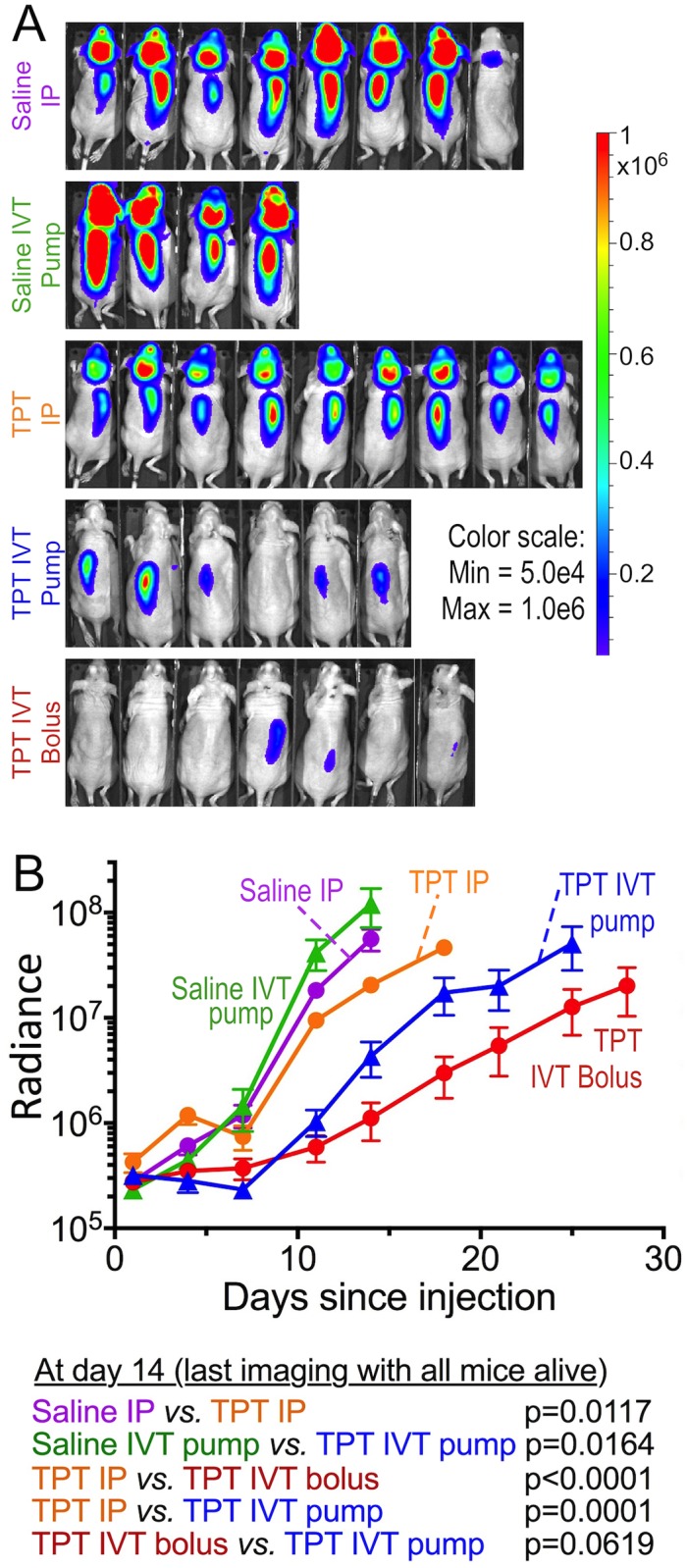
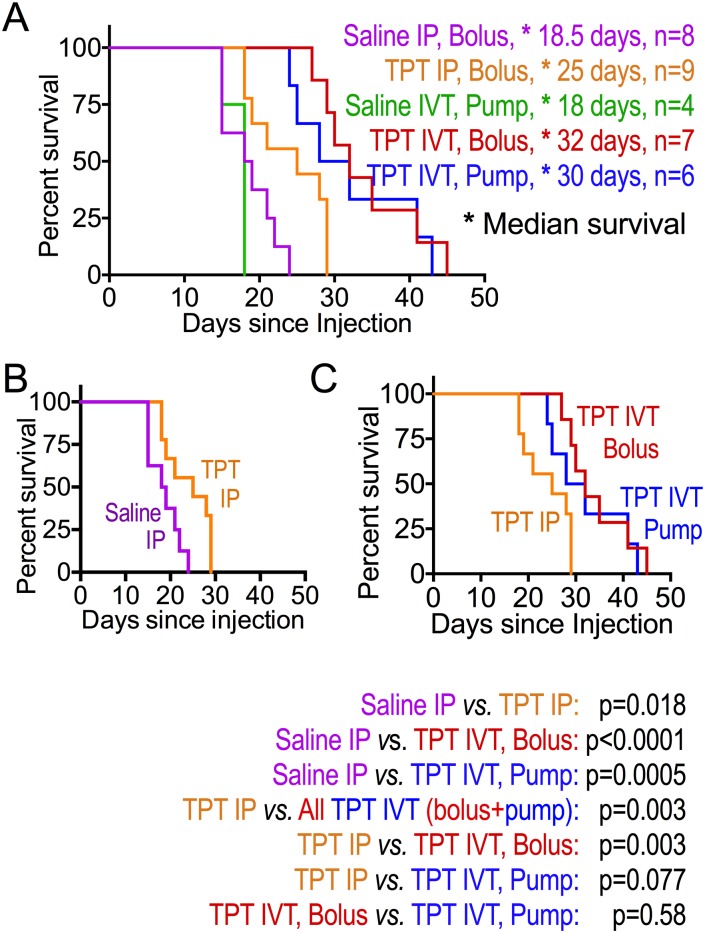
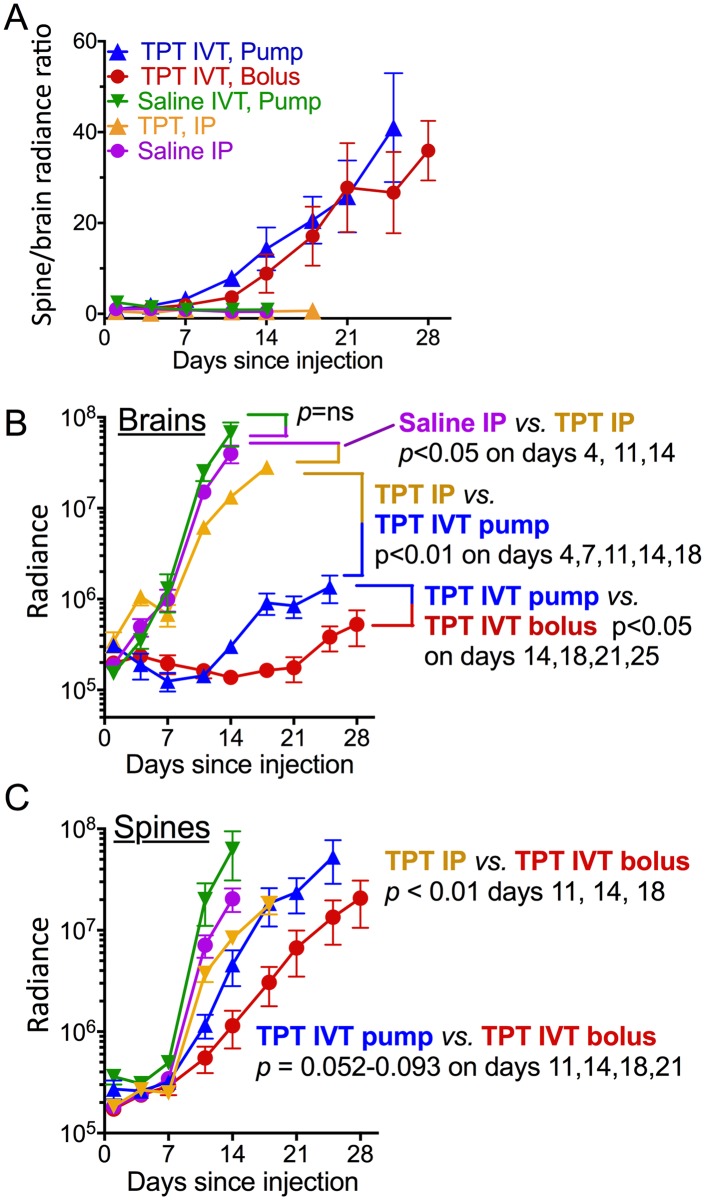
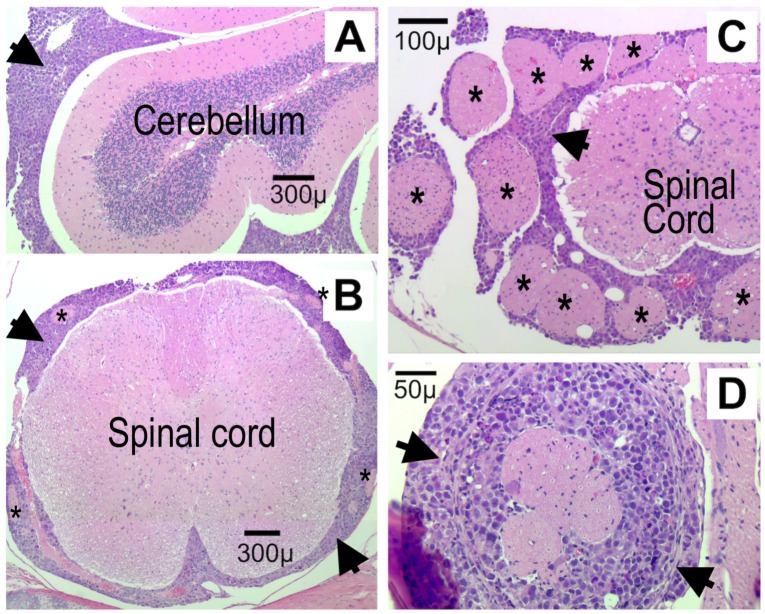
Leptomeningeal metastasis remains a difficult clinical challenge. Some success has been achieved by direct administration of therapeutics into the cerebrospinal fluid (CSF) circumventing limitations imposed by the blood brain barrier. Here we investigated continuous infusion versus bolus injection of therapy into the CSF in a preclinical model of human Group 3 medulloblastoma, the molecular subgroup with the highest incidence of leptomeningeal disease. Initial tests of selected Group 3 human medulloblastoma cell lines in culture showed that D283 Med and D425 Med were resistant to cytosine arabinoside and methotrexate. D283 Med cells were also resistant to topotecan, whereas 1 μM topotecan killed over 99% of D425 Med cells. We therefore introduced D425 Med cells, modified to express firefly luciferase, into the CSF of immunodeficient mice. Mice were then treated with topotecan or saline in five groups: continuous intraventricular (IVT) topotecan via osmotic pump (5.28 μg/day), daily bolus IVT topotecan injections with a similar daily dose (6 μg/day), systemic intraperitoneal injections of a higher daily dose of topotecan (15 μg/day), daily IVT pumped saline and daily intraperitoneal injections of saline. Bioluminescence analyses revealed that both IVT topotecan treatments effectively slowed leptomeningeal tumor growth in the brains. Histological analysis showed that they were associated with localized brain necrosis, possibly due to backtracking of topotecan around the catheter. In the spines, bolus IVT topotecan showed a trend towards slower tumor growth compared to continuous (pump) IVT topotecan, as measured by bioluminescence. Both continuous and bolus topotecan IVT showed longer survival compared to other groups. Thus, both direct IVT topotecan CSF delivery methods produced better anti-medulloblastoma effect compared to systemic therapy at the dosages used here.
脑膜转移仍然是一个具有挑战性的临床难题。通过将治疗药物直接注入脑脊液 (CSF) 绕过血脑屏障的限制,一些治疗方法取得了一定的成功。在这里,我们在人类 3 组髓母细胞瘤的临床前模型中研究了连续输注与单次注射治疗药物进入 CSF 的效果,3 组髓母细胞瘤是脑膜疾病发生率最高的分子亚型。在培养的选定的 3 组人类髓母细胞瘤细胞系的初步测试中,我们发现 D283 Med 和 D425 Med 对阿糖胞苷和甲氨蝶呤有耐药性。D283 Med 细胞也对拓扑替康有耐药性,而 1 μM 的拓扑替康杀死了超过 99%的 D425 Med 细胞。因此,我们将表达萤火虫荧光素酶的 D425 Med 细胞引入免疫缺陷小鼠的 CSF 中。然后,将小鼠分为五组,分别用拓扑替康或生理盐水进行治疗:通过渗透泵持续脑室(IVT)输注拓扑替康(5.28 μg/天)、每天 IVT 推注拓扑替康类似日剂量(6 μg/天)、腹腔内注射更高日剂量拓扑替康(15 μg/天)、每天 IVT 泵注生理盐水和每天腹腔内注射生理盐水。生物发光分析显示,两种 IVT 拓扑替康治疗均能有效减缓脑内脑膜肿瘤的生长。组织学分析表明,它们与局部脑坏死有关,可能是由于拓扑替康在导管周围回流所致。在脊柱中,与持续 IVT(泵)拓扑替康相比,单次 IVT 拓扑替康显示出肿瘤生长速度较慢的趋势,通过生物发光测量。与其他组相比,连续和单次 IVT 拓扑替康治疗均延长了生存时间。因此,与全身治疗相比,在本研究中使用的剂量下,直接 IVT 拓扑替康 CSF 给药方法产生了更好的抗髓母细胞瘤效果。