Data and Applied Science Impact, Ontario HIV Treatment Network, Toronto, Canada.
Public Health Ontario, Toronto, Canada.
PLoS One. 2019 Jan 4;14(1):e0210096. doi: 10.1371/journal.pone.0210096. eCollection 2019.
The HIV cascade is an important framework for assessing systems of care, but population-based assessment is lacking for most jurisdictions worldwide. We measured cascade indicators over time in a population-based cohort of diagnosed people living with HIV (PLWH) in Ontario, Canada.
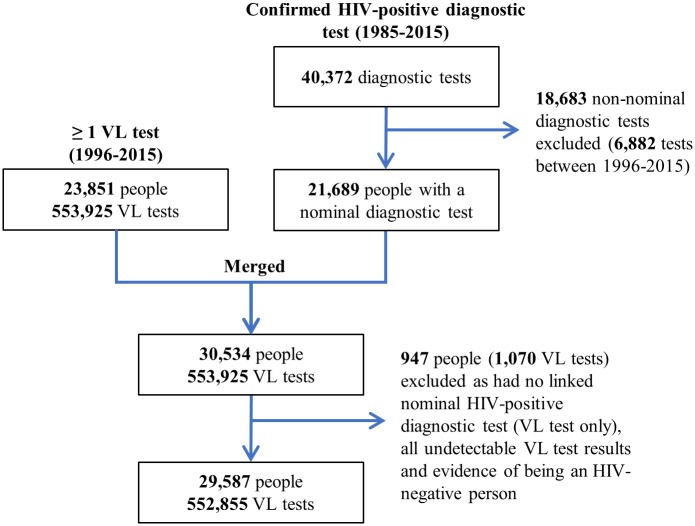
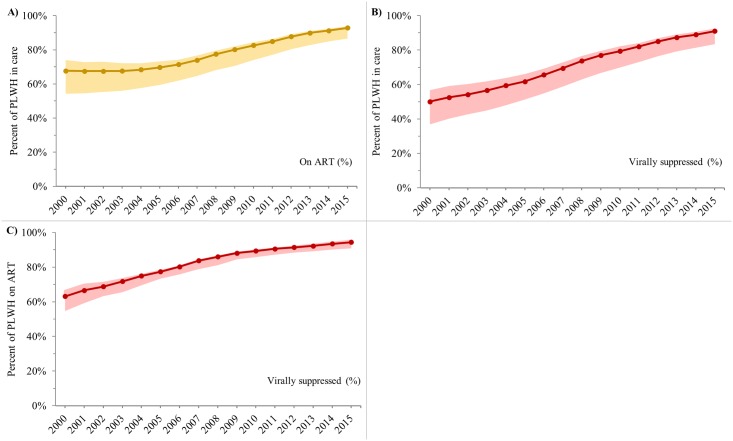
We created a retrospective cohort of diagnosed PLWH using a centralized laboratory database with HIV diagnostic and viral load (VL) test records linked at the individual-level. Individuals enter the cohort with record of a nominal HIV-positive diagnostic test or VL test, and remain unless administratively lost to follow-up (LTFU, >2 consecutive years with no VL test and no VL test in later years). We calculated the annual percent of diagnosed PLWH (cohort individuals not LTFU) between 2000 and 2015 who were in care (≥1 VL test), on ART (as documented on VL test requisition) or virally suppressed (<200 copies/ml). We also calculated time from diagnosis to linkage to care and viral suppression among individuals newly diagnosed with HIV. Analyses were stratified by sex and age. Upper/lower bounds were calculated using alternative indicator definitions.
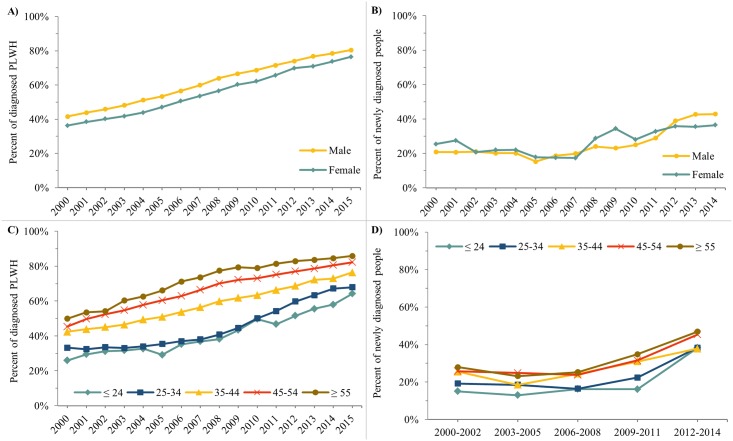
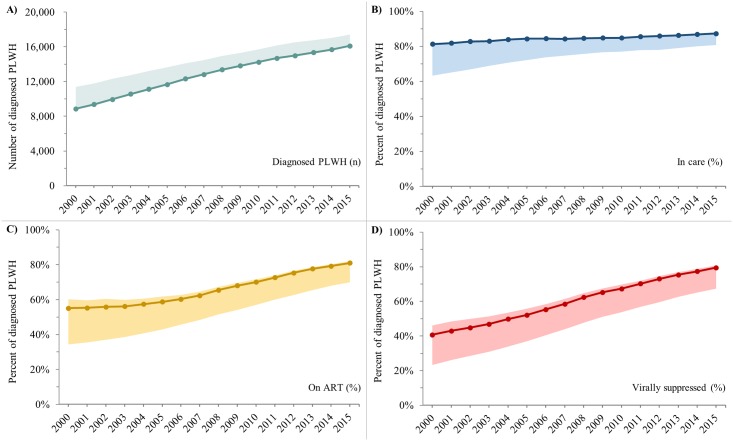
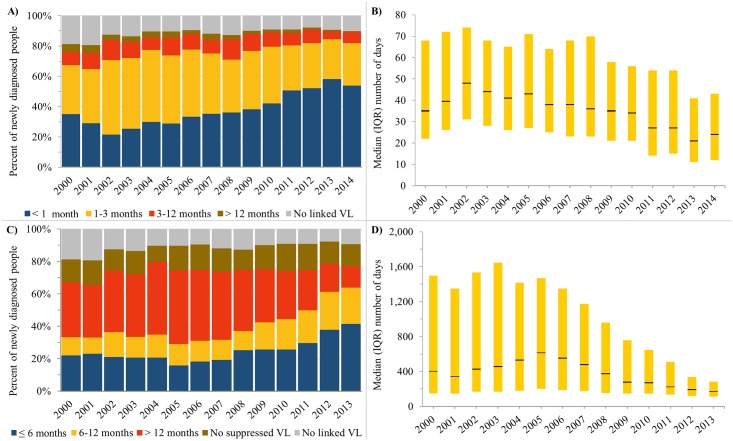
The number of diagnosed PLWH increased from 8,859 (8,859-11,389) in 2000 to 16,110 (16,110-17,423) in 2015. Over this 16-year period, the percent of diagnosed PLWH who were: in care increased from 81% (63-81%) to 87% (81-87%), on ART increased from 55% (34-60%) to 81% (70-82%) and virally suppressed increased from 41% (23-46%) to 80% (67-81%). Between 2000 and 2014, the percent of newly diagnosed individuals who linked to care within three months of diagnosis or achieved viral suppression within six months of diagnosis increased from 67% to 82% and from 22% to 42%, respectively. Estimates were generally lower for females and younger individuals.
HIV cascade indicators among diagnosed PLWH in Ontario improved between 2000 and 2015, but gaps still remain-particularly for younger individuals.
HIV 级联是评估护理系统的重要框架,但全球大多数司法管辖区都缺乏基于人群的评估。我们在加拿大安大略省的一个基于人群的确诊 HIV 感染者队列中,随着时间的推移测量了级联指标。
我们使用一个集中的实验室数据库创建了一个回顾性确诊 HIV 感染者队列,该数据库通过个体水平的 HIV 诊断和病毒载量(VL)检测记录进行链接。个体记录 HIV 阳性诊断检测或 VL 检测,除非行政上失访(LTFU,连续 2 年以上无 VL 检测且无 VL 检测)。我们计算了 2000 年至 2015 年期间,每年在诊的 HIV 感染者(队列中未失访的个体)中,处于治疗(至少有一次 VL 检测)、接受抗逆转录病毒治疗(ART)(VL 检测申请记录)或病毒抑制(<200 拷贝/ml)的比例。我们还计算了新诊断为 HIV 的个体从诊断到开始治疗和病毒抑制的时间。分析按性别和年龄分层。使用替代指标定义计算上限和下限。
确诊的 HIV 感染者人数从 2000 年的 8859 人(8859-11389 人)增加到 2015 年的 16110 人(16110-17423 人)。在这 16 年期间,处于治疗中的诊断 HIV 感染者的比例从 81%(63-81%)增加到 87%(81-87%),接受 ART 的比例从 55%(34-60%)增加到 81%(70-82%),病毒抑制的比例从 41%(23-46%)增加到 80%(67-81%)。2000 年至 2014 年,新诊断个体在诊断后三个月内开始治疗或在诊断后六个月内实现病毒抑制的比例从 67%增加到 82%,从 22%增加到 42%。女性和年轻个体的估计值通常较低。
2000 年至 2015 年,安大略省确诊 HIV 感染者的 HIV 级联指标有所改善,但差距仍然存在,尤其是年轻个体。