Dharmawan Tommy, Nakajima Tadashi, Ohno Seiko, Iizuka Takashi, Tamura Shuntaro, Kaneko Yoshiaki, Horie Minoru, Kurabayashi Masahiko
Department of Cardiovascular Medicine, Gunma University Graduate School of Medicine, Maebashi, Japan.
Department of Bioscience and Genetics, National Cerebral and Cardiovascular Center, Suita, Japan.
Ann Noninvasive Electrocardiol. 2019 May;24(3):e12623. doi: 10.1111/anec.12623. Epub 2019 Jan 7.
RYR2, encoding cardiac ryanodine receptor, is the major responsible gene for catecholaminergic polymorphic ventricular tachycardia (CPVT). Meanwhile, KCNJ2, encoding inward-rectifier potassium channel (I ), can be the responsible gene for atypical CPVT. We recently encountered a family with CPVT and sought to identify a responsible gene variant.
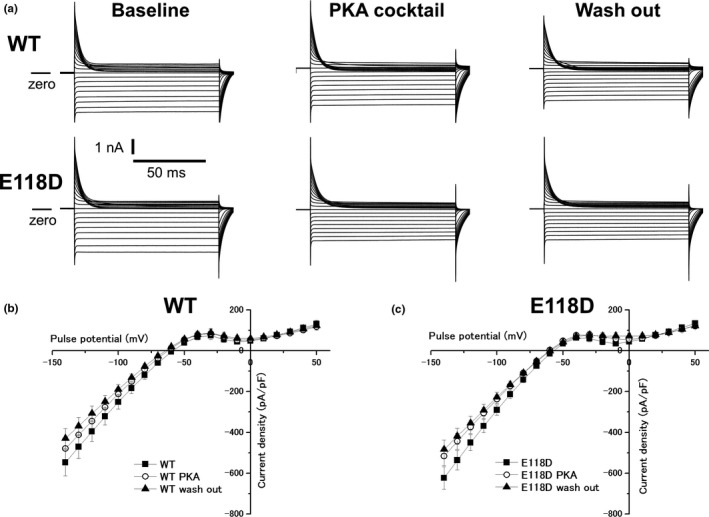
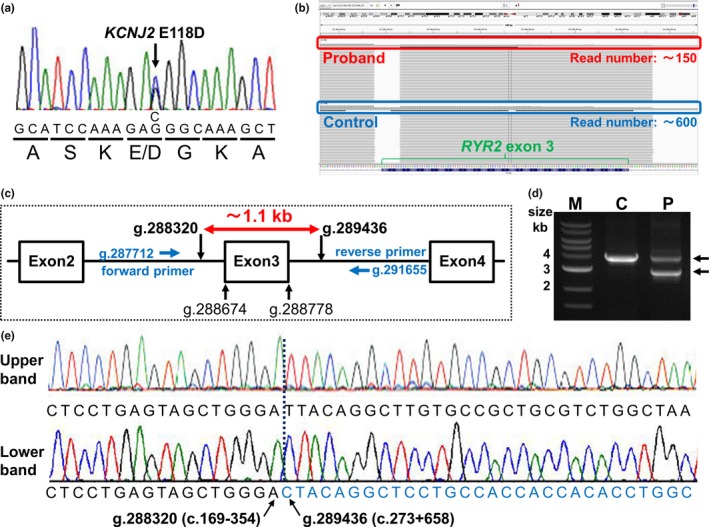
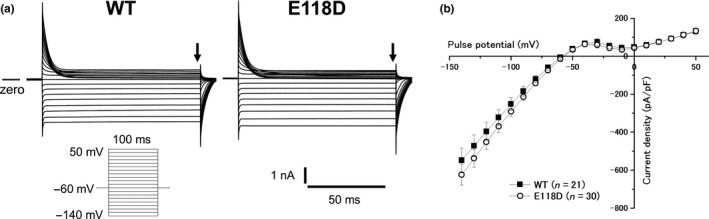
A targeted panel sequencing (TPS) was employed in the proband. Copy number variation (CNV) in RYR2 was identified by focusing on read numbers in the TPS and long-range PCR. Cascade screening was conducted by a Sanger method and long-range PCR. KCNJ2 wild-type (WT) or an identified variant was expressed in COS-1 cells, and whole-cell currents (I ) were recorded using patch-clamp techniques.
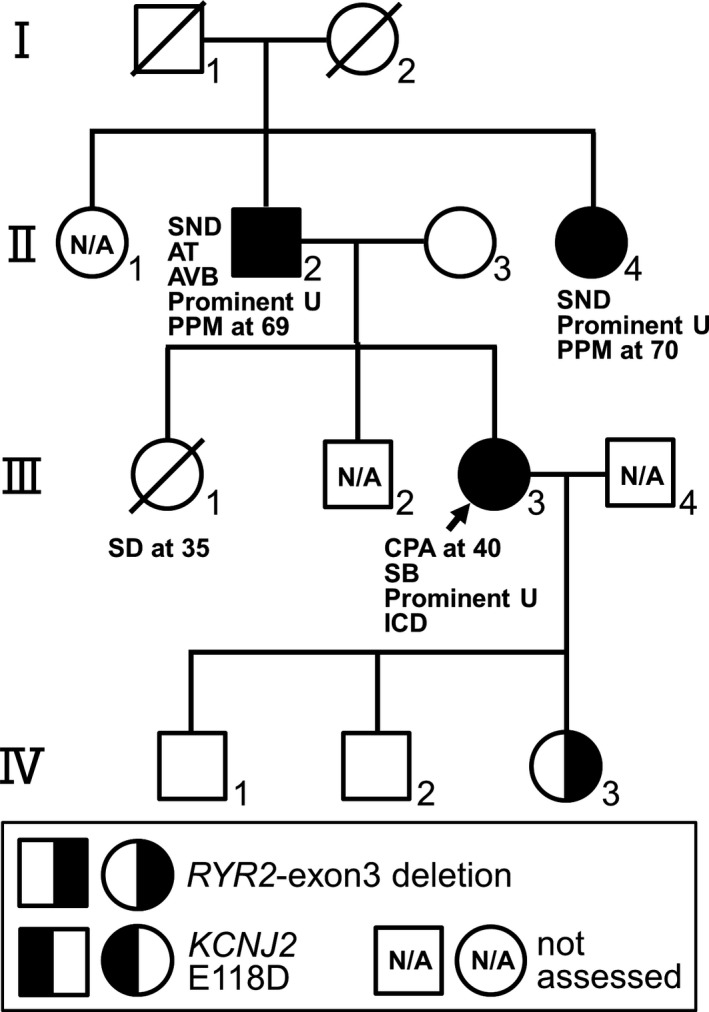
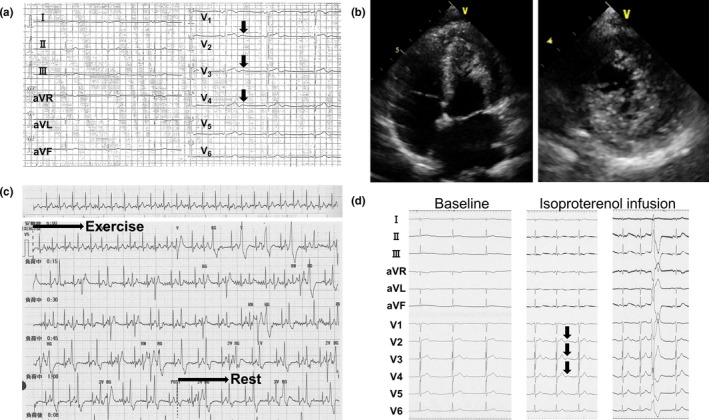
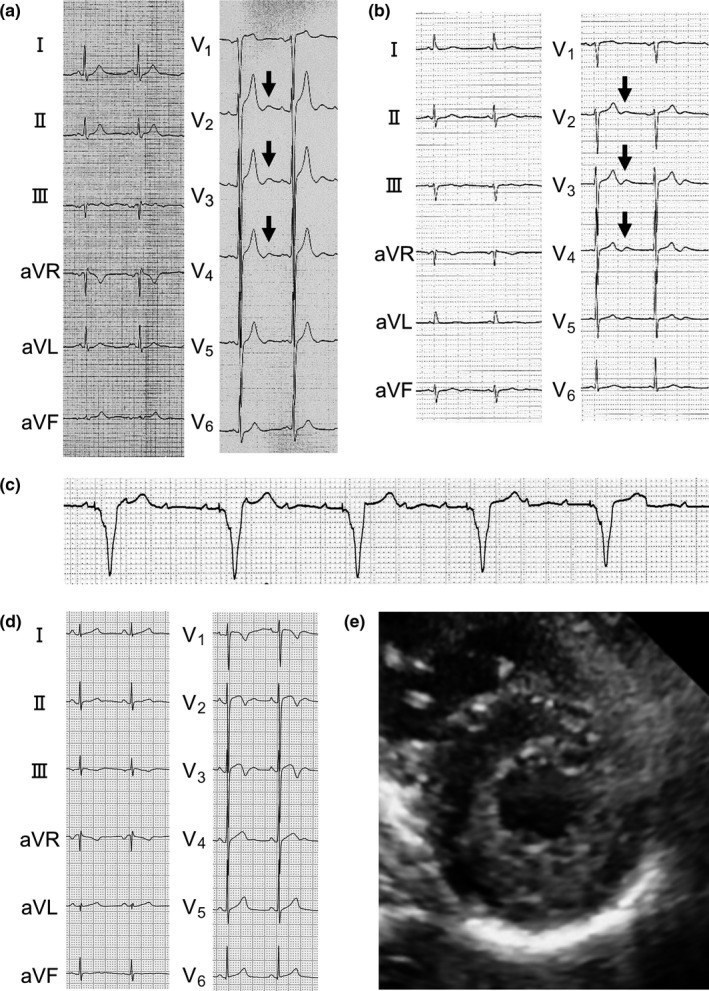
A 40-year-old female experienced cardiopulmonary arrest while cycling. Her ECG showed sinus bradycardia with prominent U-waves (≥0.2 mV). She had left ventricular hypertrabeculation at apex. Exercise induced frequent polymorphic ventricular arrhythmias. Her sister died suddenly at age 35 while bouldering. Her father and paternal aunt, with prominent U-waves, received permanent pacemaker due to sinus node dysfunction. The initial TPS and cascade screening identified a KCNJ2 E118D variant in all three symptomatic patients. However, after focusing on read numbers, we identified a novel exon3 deletion of RYR2 (RYR2-exon3 deletion) in all of them. Functional analysis revealed that KCNJ2 E118D generated I indistinguishable from KCNJ2 WT, even in the presence of catecholaminergic stimulation.
Focusing on the read numbers in the TPS enabled us to identify a novel CNV, RYR2-exon3 deletion, which was associated with phenotypic features of this family.
编码心肌兰尼碱受体的RYR2是儿茶酚胺能多形性室性心动过速(CPVT)的主要致病基因。同时,编码内向整流钾通道(I )的KCNJ2可能是不典型CPVT的致病基因。我们最近遇到一个CPVT家系,并试图鉴定致病基因变异。
对先证者进行靶向基因panel测序(TPS)。通过关注TPS中的读数和长程PCR来鉴定RYR2中的拷贝数变异(CNV)。采用Sanger法和长程PCR进行级联筛查。将KCNJ2野生型(WT)或鉴定出的变异体在COS-1细胞中表达,并使用膜片钳技术记录全细胞电流(I )。
一名40岁女性在骑自行车时发生心肺骤停。她的心电图显示窦性心动过缓伴明显U波(≥0.2mV)。她的心尖部有左心室小梁增多。运动诱发频繁的多形性室性心律失常。她的姐姐在35岁攀岩时突然死亡。她的父亲和姑姑因窦房结功能障碍有明显U波,接受了永久性起搏器植入。最初的TPS和级联筛查在所有三名有症状的患者中均鉴定出KCNJ2 E118D变异体。然而,在关注读数后,我们在所有患者中均鉴定出一种新的RYR2外显子3缺失(RYR2-外显子3缺失)。功能分析显示,即使在儿茶酚胺能刺激存在的情况下,KCNJ2 E118D产生的I 与KCNJ2 WT无明显差异。
关注TPS中的读数使我们能够鉴定出一种新的CNV,即RYR2-外显子3缺失,其与该家系的表型特征相关。