Kujawski Stephanie A, Leslie Hannah H, Prabhakaran Dorairaj, Singh Kavita, Kruk Margaret E
Department of Epidemiology, Columbia University Mailman School of Public Health, New York, New York, USA.
Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Boston, Massachusetts, USA.
BMJ Glob Health. 2018 Dec 20;3(6):e001002. doi: 10.1136/bmjgh-2018-001002. eCollection 2018.
In India, for most patients, primary healthcare remains the intended entry point for the management of non-communicable disease risk factors. The extent and determinants of non-utilisation of public primary care among households with hypertension are not well examined. We explored health facility utilisation patterns and reasons for non-utilisation of public facilities in 21 states and union territories in India, with a focus on hypertension.
We used data from the 2012-2013 District Level Household and Facility Survey. We examined the self-reported usual source of care for all households, households with hypertension and─to understand multimorbidity for those with hypertension─households with hypertension and diabetes. Hypertension was defined by self-reported diagnosis or measurement of systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg. Diabetes was defined by self-reported diagnosis or fasting blood glucose level ≥ 7.0 mmol/L or non-fasting blood glucose level ≥ 11.1 mmol/L. We assessed facility utilisation choice and reasons for non-utilisation of public facilities by household with the presence of hypertension alone and hypertension with diabetes.
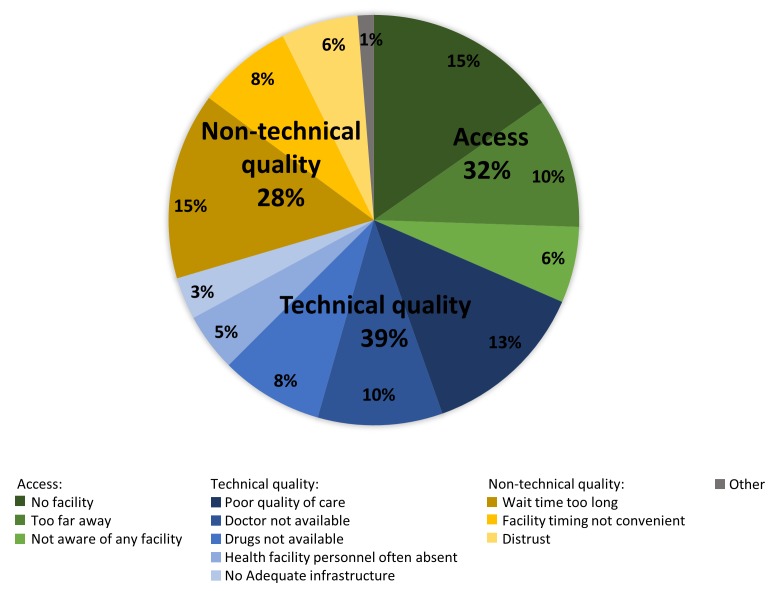
In 336 305 households, 37.6% (N=126 597) had at least one household member with hypertension, while 15.9% (N=53 385) had members with hypertension and diabetes. 20.0% of households sought care at public primary clinics, 29.9% at public hospitals and 48.3% at private facilities. Choice of private facilities increased with the burden of disease. Households with hypertension only and hypertension and diabetes cited quality reasons for non-utilisation of public facilities more than households without hypertension.
Households, particularly those with hypertension, chose private over public primary facilities for usual care. Quality of care was an important determinant of facility choice in households with hypertension and diabetes. With the increase in hypertension and cardiovascular disease in India, quality of public primary healthcare must be addressed for current policy to become reality.
在印度,对于大多数患者而言,初级医疗保健仍是管理非传染性疾病风险因素的预期切入点。高血压家庭未利用公共初级保健的程度和决定因素尚未得到充分研究。我们探讨了印度21个邦和联邦属地的卫生设施利用模式以及未利用公共设施的原因,重点关注高血压。
我们使用了2012 - 2013年地区级家庭与设施调查的数据。我们调查了所有家庭、有高血压的家庭以及——为了解高血压患者的多病共存情况——有高血压和糖尿病的家庭自我报告的常规就医来源。高血压的定义为自我报告诊断或收缩压测量值≥140毫米汞柱或舒张压测量值≥90毫米汞柱。糖尿病的定义为自我报告诊断或空腹血糖水平≥7.0毫摩尔/升或非空腹血糖水平≥11.1毫摩尔/升。我们评估了仅患有高血压的家庭以及患有高血压和糖尿病的家庭对设施利用的选择以及未利用公共设施的原因。
在336305个家庭中,37.6%(N = 126597)至少有一名家庭成员患有高血压,而15.9%(N = 53385)有成员患有高血压和糖尿病。20.0%的家庭在公共初级诊所就医,29.9%在公立医院就医,48.3%在私立机构就医。对私立机构的选择随着疾病负担的增加而增加。仅患有高血压的家庭以及患有高血压和糖尿病的家庭比没有高血压的家庭更多地以质量为由未利用公共设施。
家庭,尤其是那些患有高血压的家庭,在常规就医时选择私立初级设施而非公共设施。医疗质量是患有高血压和糖尿病家庭选择设施的重要决定因素。随着印度高血压和心血管疾病的增加,要使当前政策成为现实,就必须解决公共初级医疗保健的质量问题。