Luan Erfe Betty M, Boehme Jacqueline, Erfe J Mark, Brovman Ethan Y, Bader Angela M, Urman Richard D
Harvard Medical School, Boston, MA, USA.
Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women's Hospital, Boston, MA, USA.
Geriatr Orthop Surg Rehabil. 2018 Dec 21;9:2151459318816482. doi: 10.1177/2151459318816482. eCollection 2018.
To evaluate the body of evidence on the predictive value of preoperative cognitive impairment on in-hospital, short-term, and midterm postoperative outcomes for elderly patients undergoing total knee arthroplasty (TKA).
With an aging population, an increasing percentage of the U.S. patient population will be living with cognitive impairment. There is currently no systematic review that assesses postoperative outcomes of patients with mild cognitive impairment (MCI) or preexisting diagnosis of dementia while undergoing elective primary TKA.
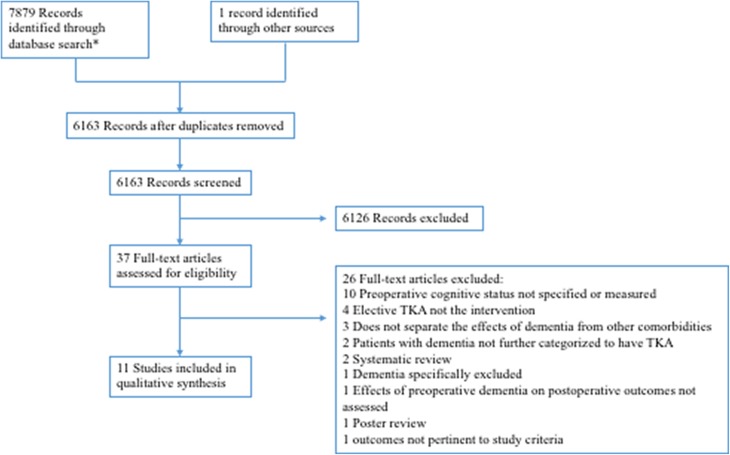
A database search between January 1, 1997, and November 1, 2017 in EMBASE, MEDLINE, and PubMed was conducted to identify articles that compared postoperative outcomes after TKA between patients aged 60 years with and without cognitive impairment. Cognitive impairment included preexisting diagnosis of dementia or MCI identified during preoperative assessment. Eligible articles were selected using dual reviewer and third-party arbitrator. The quality of the studies was evaluated using the Newcastle-Ottawa Scale. The strength of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation approach. A total of 6163 abstracts were screened. Only 11 full text articles met inclusion criteria, including 1 case-control, 5 prospective cohort, and 5 retrospective cohort studies. Two studies were of poor quality. Overall, there is moderate strength of evidence for increased risk of postoperative delirium, increased length of stay, and discharge to health-care facility among patients with preoperative MCI or preexisting dementia. The body of evidence is weak for other outcomes of interest including mortality, functionality and complications while in-hospital and in the short- and midterm.
This review highlights the need for additional good quality studies to provide more information about MCI and dementia as risk factors in primary TKA.
评估术前认知障碍对接受全膝关节置换术(TKA)的老年患者院内、短期和中期术后结局的预测价值的证据。
随着人口老龄化,美国认知障碍患者的比例将不断增加。目前尚无系统评价评估轻度认知障碍(MCI)患者或术前已诊断为痴呆的患者在接受择期初次TKA时的术后结局。
在1997年1月1日至2017年11月1日期间,对EMBASE、MEDLINE和PubMed数据库进行检索,以确定比较60岁有认知障碍和无认知障碍患者TKA术后结局的文章。认知障碍包括术前评估时已诊断的痴呆或MCI。采用双审核员和第三方仲裁员选择符合条件的文章。使用纽卡斯尔-渥太华量表评估研究质量。采用推荐分级评估、发展和评价方法评估证据强度。共筛选6163篇摘要。只有11篇全文文章符合纳入标准,包括1篇病例对照研究、5篇前瞻性队列研究和5篇回顾性队列研究。两项研究质量较差。总体而言,有中等强度的证据表明,术前MCI或已患痴呆的患者术后谵妄风险增加、住院时间延长以及出院至医疗机构的比例增加。对于其他感兴趣的结局,包括住院期间以及短期和中期的死亡率、功能和并发症,证据不足。
本综述强调需要更多高质量的研究,以提供更多关于MCI和痴呆作为初次TKA危险因素的信息。