Department of Nutrition, University of California, Davis, Davis, CA.
Division of Epidemiology and Biostatistics, University of California, Berkeley, Berkeley, CA.
Am J Clin Nutr. 2019 Jan 1;109(1):148-164. doi: 10.1093/ajcn/nqy239.
Anemia in young children is a global health problem. Risk factors include poor nutrient intake and poor water quality, sanitation, or hygiene.
We evaluated the effects of water quality, sanitation, handwashing, and nutrition interventions on micronutrient status and anemia among children in rural Kenya and Bangladesh.
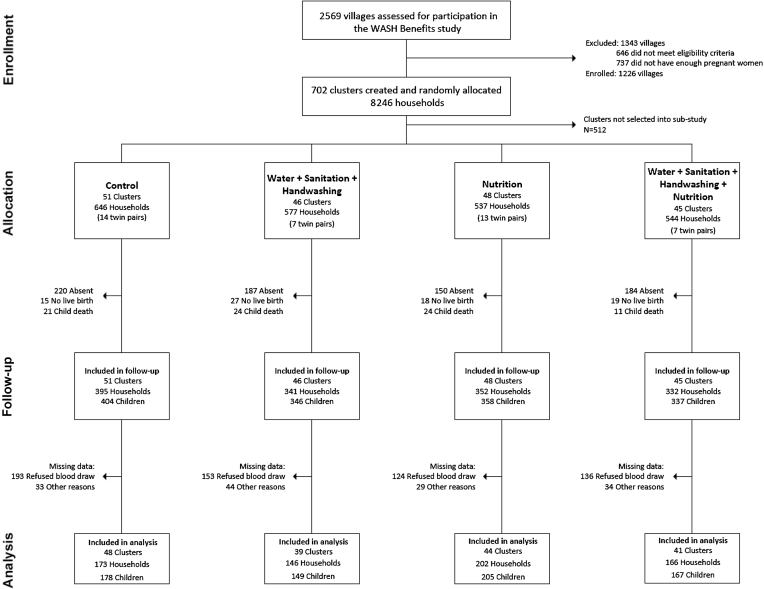
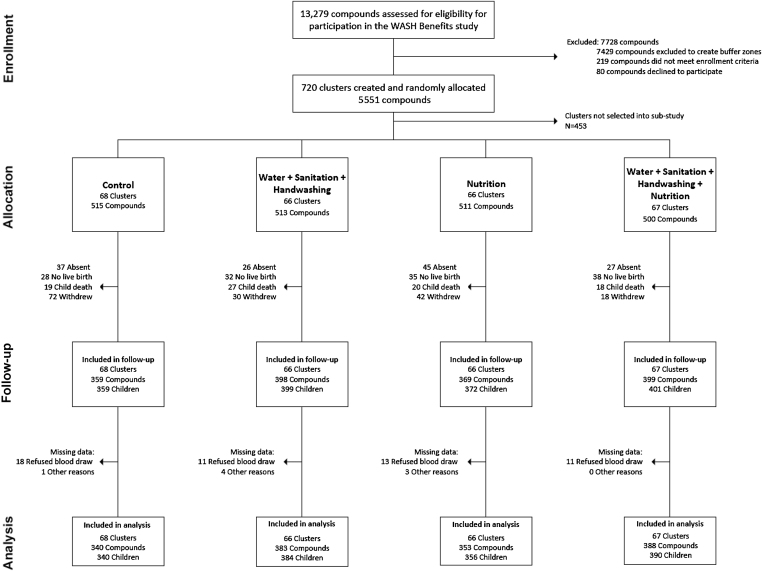
We nested substudies within 2 cluster-randomized controlled trials enrolling pregnant women and following their children for 2 y. These substudies included 4 groups: water, sanitation, and handwashing (WSH); nutrition (N), including lipid-based nutrient supplements (LNSs; ages 6-24 mo) and infant and young child feeding (IYCF) counseling; WSH+N; and control. Hemoglobin and micronutrient biomarkers were measured after 2 y of intervention and compared between groups using generalized linear models with robust SEs.
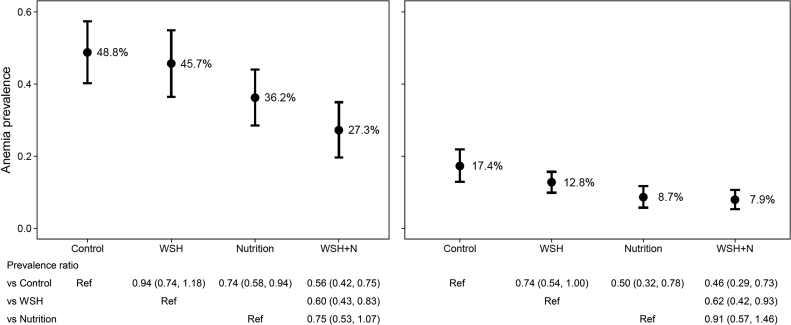
In Kenya, 699 children were assessed at a mean ± SD age of 22.1 ± 1.8 mo, and in Bangladesh 1470 participants were measured at a mean ± SD age of 28.0 ± 1.9 mo. The control group anemia prevalences were 48.8% in Kenya and 17.4% in Bangladesh. There was a lower prevalence of anemia in the 2 N intervention groups in both Kenya [N: 36.2%; prevalence ratio (PR): 0.74; 95% CI: 0.58, 0.94; WSH+N: 27.3%; PR: 0.56; 95% CI: 0.42, 0.75] and Bangladesh (N: 8.7%; PR: 0.50; 95% CI: 0.32, 0.78; WSH+N: 7.9%, PR: 0.46; 95% CI: 0.29, 0.73). In both trials, the 2 N groups also had significantly lower prevalences of iron deficiency, iron deficiency anemia, and low vitamin B-12 and, in Kenya, a lower prevalence of folate and vitamin A deficiencies. In Bangladesh, the WSH group had a lower prevalence of anemia (12.8%; PR: 0.74; 95% CI: 0.54, 1.00) than the control group, whereas in Kenya, the WSH+N group had a lower prevalence of anemia than did the N group (PR: 0.75; 95% CI: 0.53, 1.07), but this was not significant (P = 0.102).
IYCF counseling with LNSs reduced the risks of anemia, iron deficiency, and low vitamin B-12. Effects on folate and vitamin A varied between studies. Improvements in WSH also reduced the risk of anemia in Bangladesh but did not provide added benefit over the nutrition-specific intervention. These trials were registered at clinicaltrials.gov as NCT01590095 (Bangladesh) and NCT01704105 (Kenya).
儿童贫血是一个全球性的健康问题。危险因素包括营养摄入不良和水质差、环境卫生和个人卫生差。
我们评估了水质、环境卫生、洗手和营养干预措施对肯尼亚和孟加拉国农村儿童微量营养素状况和贫血的影响。
我们在两项随机对照试验中嵌套了子研究,纳入了孕妇,并对其子女进行了 2 年的随访。这些子研究包括 4 组:水、环境卫生和洗手(WSH);营养(N),包括脂类营养素补充剂(LNSs;6-24 月龄)和婴幼儿喂养(IYCF)咨询;WSH+N;和对照组。在干预 2 年后测量血红蛋白和微量营养素生物标志物,并使用广义线性模型和稳健 SE 比较组间差异。
在肯尼亚,699 名儿童在平均年龄 22.1±1.8 个月时进行了评估,在孟加拉国,1470 名参与者在平均年龄 28.0±1.9 个月时进行了测量。对照组在肯尼亚的贫血患病率为 48.8%,在孟加拉国为 17.4%。在肯尼亚,2 个 N 干预组的贫血患病率较低[N:36.2%;患病率比(PR):0.74;95%CI:0.58,0.94;WSH+N:27.3%;PR:0.56;95%CI:0.42,0.75]和孟加拉国(N:8.7%;PR:0.50;95%CI:0.32,0.78;WSH+N:7.9%,PR:0.46;95%CI:0.29,0.73)。在这两项试验中,2 个 N 组的铁缺乏、缺铁性贫血和维生素 B-12 缺乏的患病率也明显较低,而且在肯尼亚,叶酸和维生素 A 缺乏的患病率也较低。在孟加拉国,WSH 组的贫血患病率(12.8%;PR:0.74;95%CI:0.54,1.00)低于对照组,而在肯尼亚,WSH+N 组的贫血患病率(PR:0.75;95%CI:0.53,1.07)低于 N 组,但差异无统计学意义(P=0.102)。
IYCF 咨询与 LNS 一起降低了贫血、缺铁和维生素 B-12 缺乏的风险。叶酸和维生素 A 的影响在两项研究中有所不同。WSH 的改善也降低了孟加拉国的贫血风险,但与营养特异性干预相比,没有提供额外的益处。这些试验在 clinicaltrials.gov 上注册,分别为 NCT01590095(孟加拉国)和 NCT01704105(肯尼亚)。