Webber Ann L, Wood Joanne M, Thompson Benjamin, Birch Eileen E
School of Optometry & Vision Science and Institute of Health & Biomedical Innovation, Queensland University of Technology, Brisbane, Australia.
School of Optometry and Vision Science, University of Waterloo, Waterloo, Canada.
Ophthalmic Physiol Opt. 2019 Jan;39(1):53-62. doi: 10.1111/opo.12599.
This study aimed to validate a binocular function score that is based on common clinical measures of visual function, providing a more complete analysis of binocular outcomes, against laboratory-based dichoptic tests of threshold stereoacuity and depth of suppression.
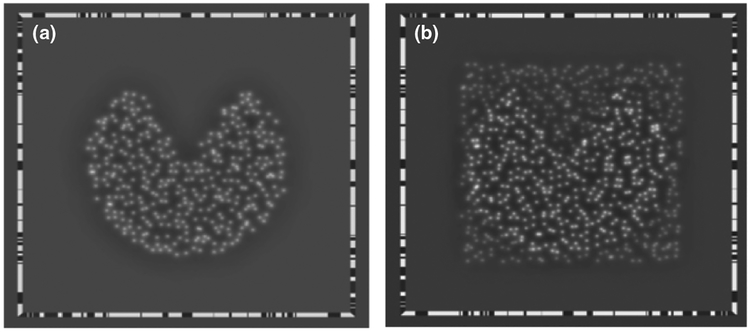
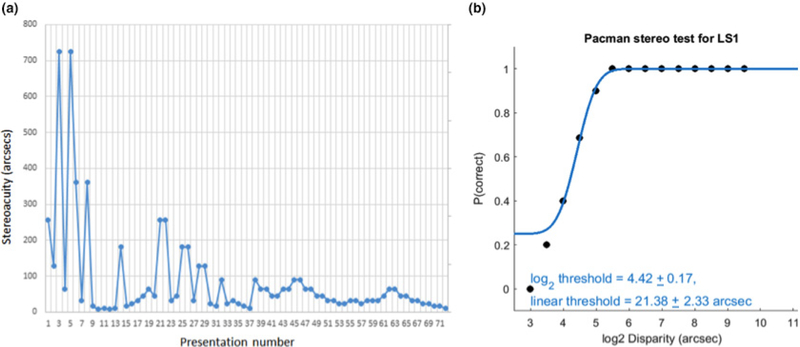
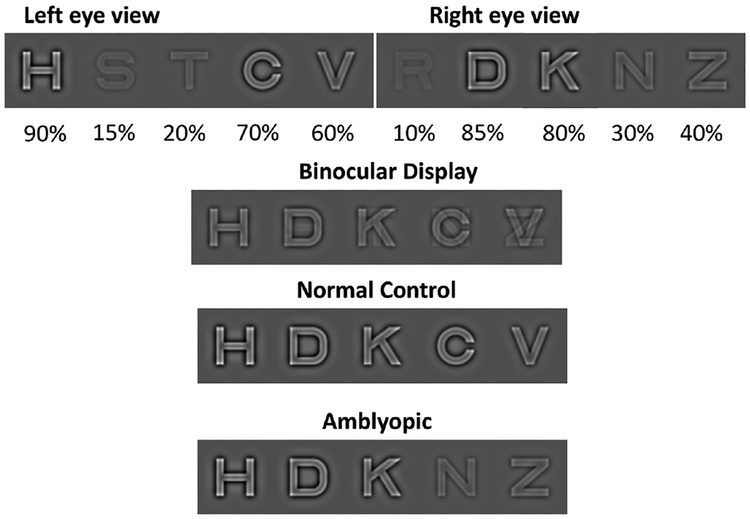
Scores on a composite binocular function (BF) score derived from clinical stereoacuity measures (Randot Preschool Stereoacuity Test and Randot Butterfly) and the Worth 4 Dot test were determined in adults (n = 20; age 24.8 ± 7.2 years) and children (N = 77; age 8.3 ± 1.7 years) with abnormal binocular vision from strabismus or amblyopia. Adults had threshold stereoacuity measured with a novel, computerised dichoptic psychophysical test of stereopsis. Depth of suppression (dichoptic eye chart inter-ocular contrast balance test) was determined in both adults and children.
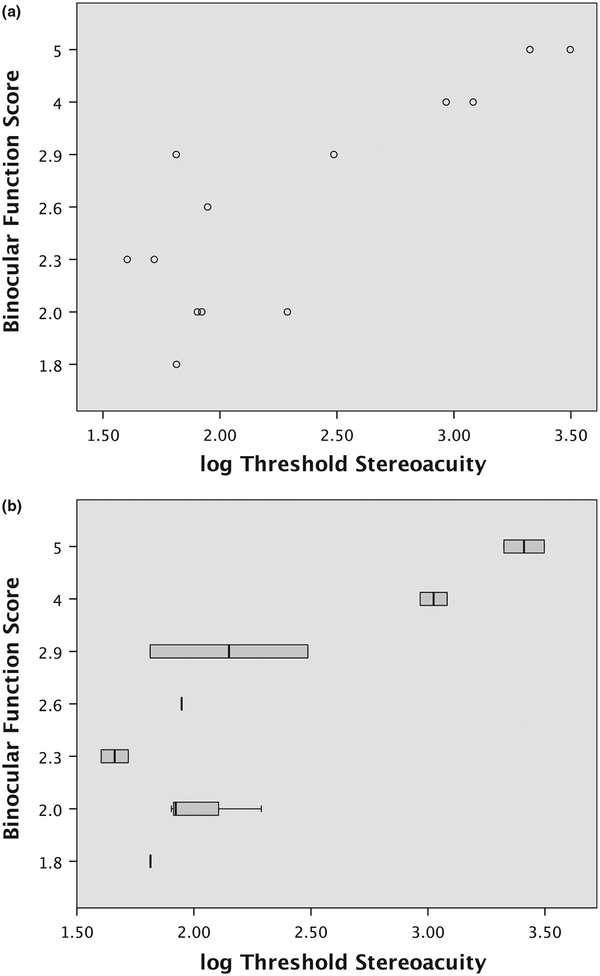
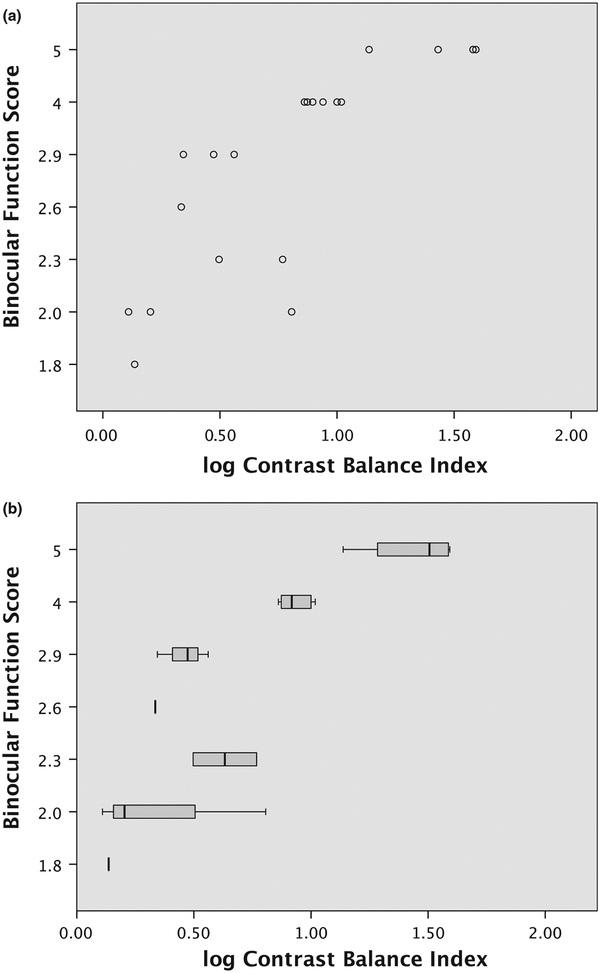
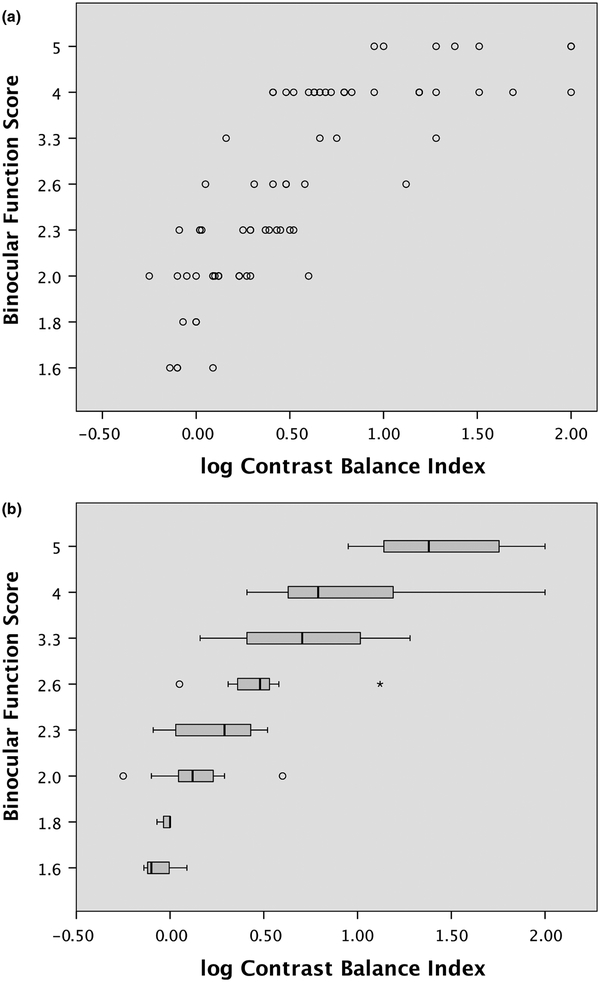
Clinical Randot stereoacuity was measurable in 50% of adult and 61% of child participants. Threshold stereoacuity was measurable in 65% of the adult participants. The presence of suppression or simultaneous perception (flat fusion or diplopia) was measurable in all participants, enabling assignment of a BF score to all participants in both groups. In adults, the BF score was highly correlated with the psychophysical threshold stereoacuity measure (ρ = 0.71; p < 0.001). In both adults and children, there was also a high correlation between the BF score and inter-ocular contrast balance (adult ρ = 0.90; child ρ = 0.86; p < 0.001).
The composite BF score is a convenient and valid scale of binocularity that can be used to extend the stereoacuity measure in cohorts where nil stereoacuity is common and thus could be considered as an outcome measure in clinical trials.
本研究旨在验证一种基于视觉功能常见临床测量的双眼功能评分,相对于基于实验室的阈值立体视锐度和抑制深度的双眼分视测试,该评分能对双眼结果进行更全面的分析。
在患有斜视或弱视导致双眼视觉异常的成人(n = 20;年龄24.8 ± 7.2岁)和儿童(N = 77;年龄8.3 ± 1.7岁)中,确定从临床立体视锐度测量(兰多学前立体视锐度测试和兰多蝴蝶测试)及沃思四点测试得出的综合双眼功能(BF)评分。使用一种新型的计算机化双眼分视心理物理学立体视测试测量成人的阈值立体视锐度。在成人和儿童中均测定抑制深度(双眼分视视力表眼间对比度平衡测试)。
50%的成年参与者和61%的儿童参与者可测量临床兰多立体视锐度。65%的成年参与者可测量阈值立体视锐度。所有参与者均可测量抑制或同时感知(平面融合或复视)的存在情况,从而能够为两组的所有参与者分配BF评分。在成人中,BF评分与心理物理学阈值立体视锐度测量高度相关(ρ = 0.71;p < 0.001)。在成人和儿童中,BF评分与眼间对比度平衡之间也存在高度相关性(成人ρ = 0.90;儿童ρ = 0.86;p < 0.001)。
综合BF评分是一种方便且有效的双眼功能量表,可用于在常见无立体视锐度的队列中扩展立体视锐度测量,因此可被视为临床试验中的一项结果指标。