Connor S E J, Dudau C, Pai I, Gaganasiou M
School of Biomedical Engineering and Imaging Sciences Clinical Academic Group, King's College, London, UK.
Department of Radiology, Guy's and St. Thomas' Hospital, London, UK.
Eur Arch Otorhinolaryngol. 2019 Mar;276(3):693-702. doi: 10.1007/s00405-019-05279-x. Epub 2019 Jan 11.
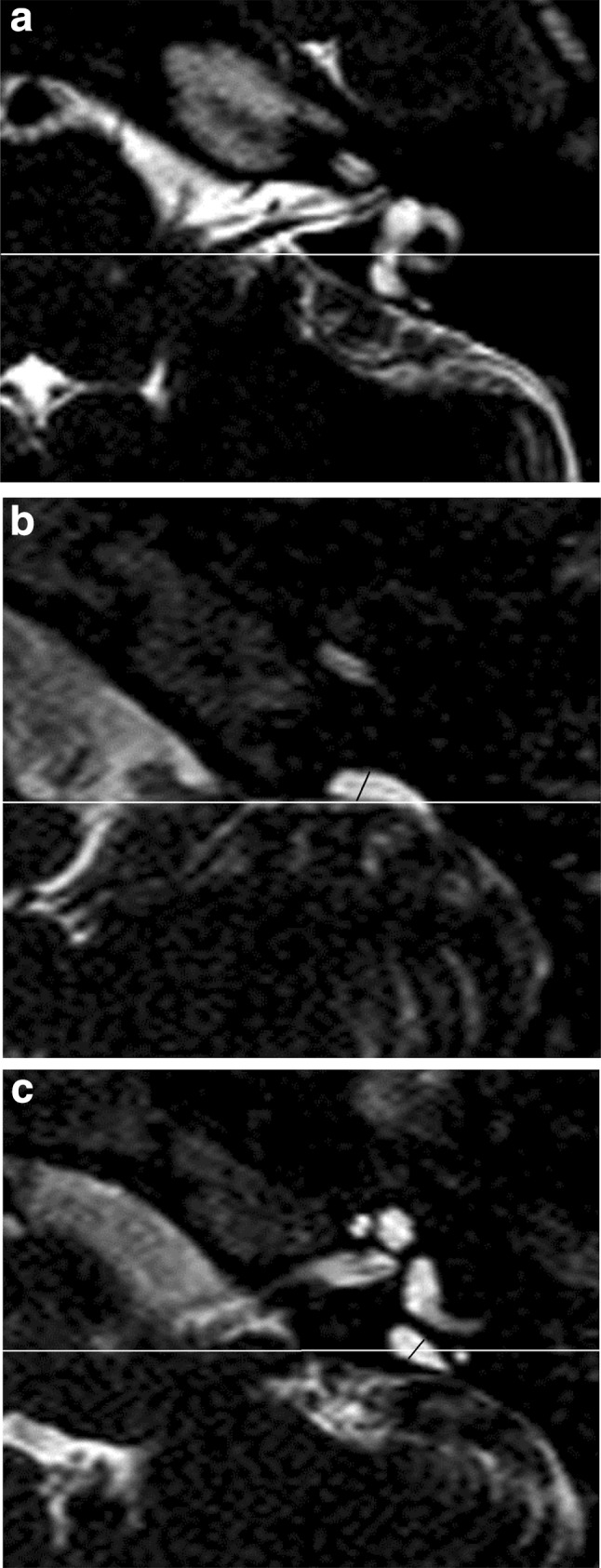
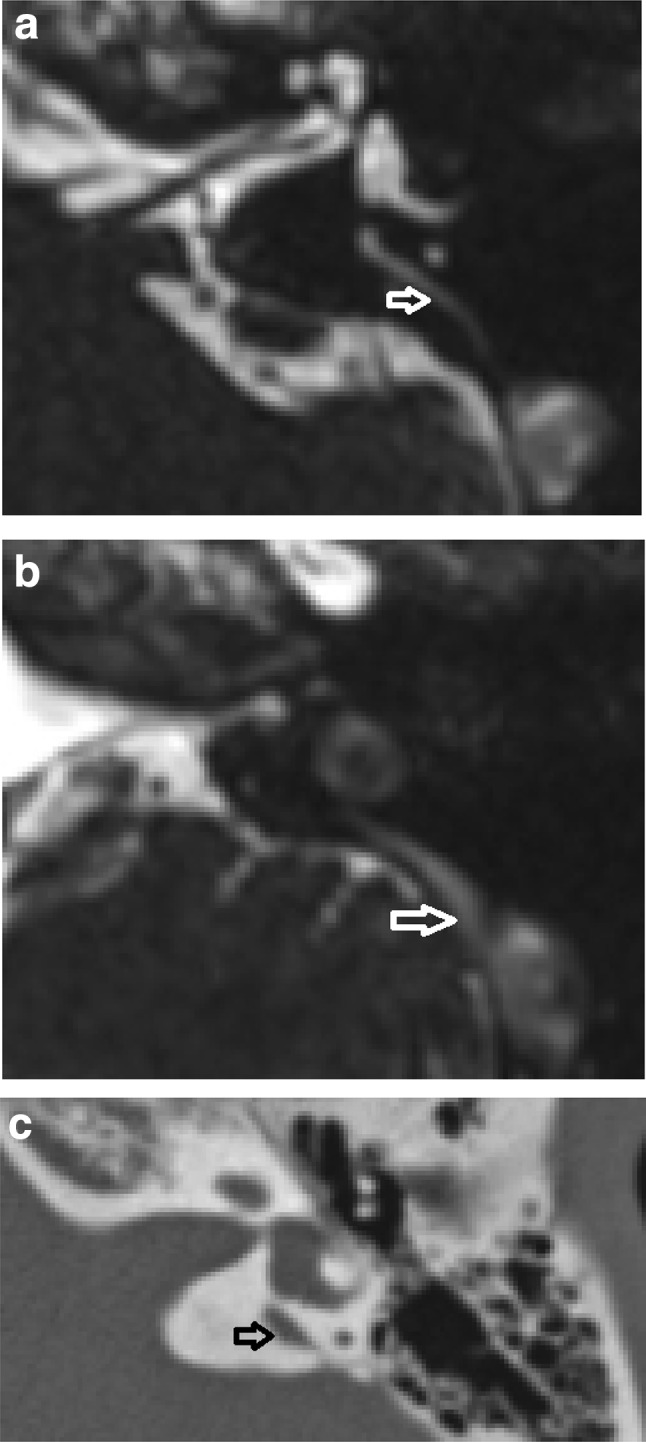
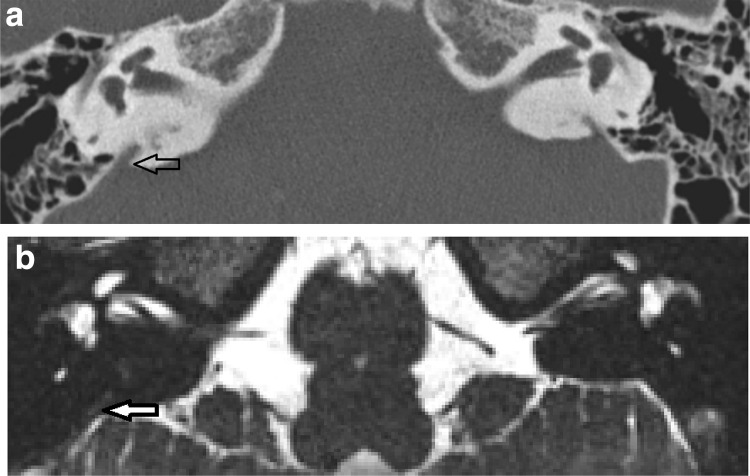
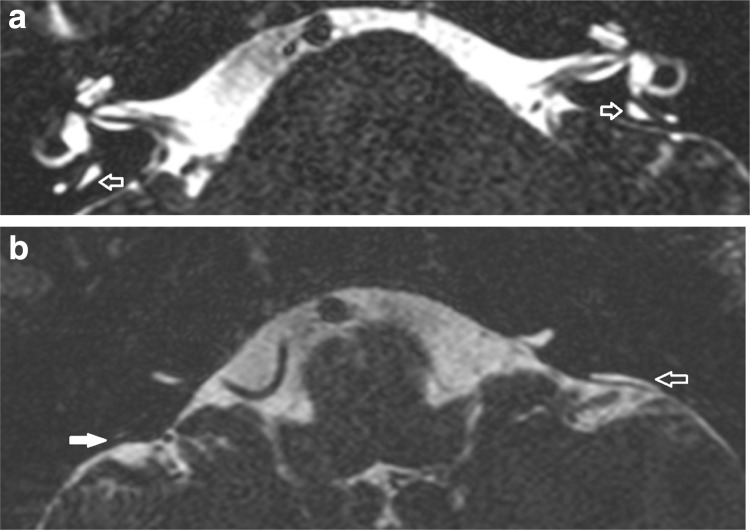
We explored whether there was a difference between measurements obtained with CT and MRI for the diagnosis of large vestibular aqueduct syndrome or large endolymphatic sac anomaly, and whether this influenced diagnosis on the basis of previously published threshold values (Valvassori and Cincinnati). We also investigated whether isolated dilated extra-osseous endolymphatic sac occurred on MRI. Secondary objectives were to compare inter-observer reproducibility for the measurements, and to investigate any mismatch between the diagnoses using the different criteria.
MATERIALS/METHODS: Subjects diagnosed with large vestibular aqueduct syndrome or large endolymphatic sac anomalies were retrospectively analysed. For subjects with both CT and MRI available (n = 58), two independent observers measured the midpoint and operculum widths. For subjects with MRI (± CT) available (n = 84), extra-osseous sac widths were also measured. Results There was no significant difference between the width measurements obtained with CT versus MRI. CT alone diagnosed large vestibular aqueduct syndrome or large endolymphatic sac anomalies in 2/58 (Valvassori) and 4/58 (Cincinnati), whilst MRI alone diagnosed them in 2/58 (Valvassori). There was 93% CT/MRI diagnostic agreement using both criteria. Only 1/84 demonstrated isolated extra-osseous endolymphatic sac dilatation. The MRI-based LVAS/LESA diagnosis was less dependent on which criteria were used. Midpoint measurements are more reproducible between observers and between CT/MR imaging modalities.
Supplementing MRI with CT results in additional diagnoses using either criterion, however, there is no net increased diagnostic sensitivity for CT versus MRI when applying the Valvassori criteria. Isolated enlargement of the extra-osseous endolymphatic sac is rare.
我们探讨了CT和MRI测量结果在诊断大前庭导水管综合征或大内淋巴囊异常方面是否存在差异,以及这是否会基于先前公布的阈值(瓦尔瓦索里和辛辛那提标准)影响诊断。我们还研究了MRI上是否出现孤立性扩张的骨外内淋巴囊。次要目的是比较观察者间测量的可重复性,并研究使用不同标准时诊断之间的任何不匹配情况。
材料/方法:对诊断为大前庭导水管综合征或大内淋巴囊异常的受试者进行回顾性分析。对于同时有CT和MRI的受试者(n = 58),两名独立观察者测量中点和壶腹宽度。对于有MRI(±CT)的受试者(n = 84),还测量骨外囊宽度。结果CT和MRI获得的宽度测量结果之间无显著差异。仅CT根据瓦尔瓦索里标准诊断出2/58例大前庭导水管综合征或大内淋巴囊异常,根据辛辛那提标准诊断出4/58例,而仅MRI根据瓦尔瓦索里标准诊断出2/58例。使用两种标准时,CT/MRI诊断一致性为93%。仅1/84例显示孤立性骨外内淋巴囊扩张。基于MRI的大前庭导水管综合征/大内淋巴囊异常诊断对所使用的标准依赖性较小。中点测量在观察者之间以及CT/MR成像方式之间更具可重复性。
CT补充MRI会根据任一标准增加额外诊断,然而,应用瓦尔瓦索里标准时,CT与MRI相比诊断敏感性并无净增加。骨外内淋巴囊的孤立性增大很少见。