Department of Neurology, General Hospital of Shen-Yang Military Region, Shenyang, China.
Stroke Vasc Neurol. 2018 Sep 23;3(4):263-267. doi: 10.1136/svn-2018-000148. eCollection 2018 Dec.
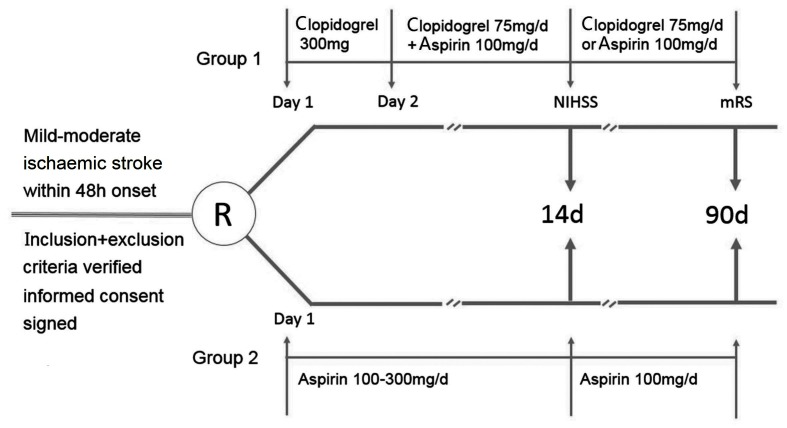
A recent study shows that dual antiplatelet therapy with clopidogrel plus aspirin is superior to aspirin monotherapy for minor stroke, which is defined as a National Institutes of Health Stroke Scale (NIHSS)score of ≤3. However, acute mild-moderate ischaemic stroke (4≤NIHSS≤10) still needs aggressive antiplatelet intervention to prevent deterioration and recurrence of stroke. The efficacy and safety of dual antiplatelet therapy versus aspirin monotherapy in the population are not clear. A multicentre clinical trial is designed to evaluate the efficacy and safety of clopidogrel plus aspirin therapy versus aspirin monotherapy within 48 hours of symptom onset of mild-moderate ischaemic stroke.
METHODS/DESIGN: The study is a randomised, open-label, multicentre, prospective trial with a target enrolment of 2700 patients from 60 centres in Northeast China. A treatment allocation identification number to each enrolled patient will be provided by a random number generator. The follow-up time for the clopidogrel plus aspirin and aspirin monotherapy groups is 90 days. The primary efficacy endpoint is a stroke progression event, which is defined as ≥4 point increase in the NIHSS score in 48 hours. The second efficacy endpoints include new ischaemic stroke within 90 days, change in the NIHSS score within 14 days, modified Rankin Scale score on day 90 and other vascular or death events within 90 days. The safety endpoints include mucocutaneous haemorrhage, organ haemorrhage and intracranial haemorrhage, adverse events and severe adverse events. χ test, t-test (or Mann-Whitney test), survival analysis and Cox proportional hazards models will be conducted. The findings of the study may provide an important evidence for clinical practice for these patients.
The trial will be conducted under a rational design and will provide valuable evidence on the appropriate treatment for this population.
The study was reviewed and approved by the Ethics Committee of the General Hospital of Shen-Yang Military Region (no K(2016) 6).
NCT02869009; Pre-results.
最近的一项研究表明,氯吡格雷联合阿司匹林双联抗血小板治疗优于阿司匹林单药治疗轻度卒中,轻度卒中指美国国立卫生研究院卒中量表(NIHSS)评分≤3 分。然而,急性轻中度缺血性卒中(4≤NIHSS≤10)仍需要积极的抗血小板干预,以防止卒中恶化和复发。双联抗血小板治疗与阿司匹林单药治疗在该人群中的疗效和安全性尚不清楚。一项多中心临床试验旨在评估氯吡格雷联合阿司匹林治疗与阿司匹林单药治疗在轻中度缺血性卒中发病后 48 小时内的疗效和安全性。
方法/设计:这是一项随机、开放标签、多中心、前瞻性试验,计划在东北地区的 60 个中心招募 2700 名患者。每位入组患者将由随机数发生器提供一个治疗分配识别号。氯吡格雷联合阿司匹林组和阿司匹林单药组的随访时间为 90 天。主要疗效终点是卒中进展事件,定义为 48 小时内 NIHSS 评分增加≥4 分。次要疗效终点包括 90 天内新发缺血性卒中、14 天内 NIHSS 评分变化、90 天改良 Rankin 量表评分和 90 天内其他血管或死亡事件。安全性终点包括黏膜出血、器官出血和颅内出血、不良事件和严重不良事件。将进行 χ 检验、t 检验(或 Mann-Whitney 检验)、生存分析和 Cox 比例风险模型。该研究的结果可能为这些患者的临床实践提供重要证据。
该试验将在合理的设计下进行,并将为该人群的适当治疗提供有价值的证据。
该研究已由沈阳军区总医院伦理委员会审查和批准(编号 K(2016)6)。
NCT02869009;预注册。