Department of Surgical Oncology, Erasmus MC Cancer Institute, P.O. Box 2040, 3000 CA, Rotterdam, The Netherlands.
Department of Surgery, Erasmus Medical Centre, Rotterdam, The Netherlands.
Angiogenesis. 2019 May;22(2):355-368. doi: 10.1007/s10456-019-09661-5. Epub 2019 Jan 12.
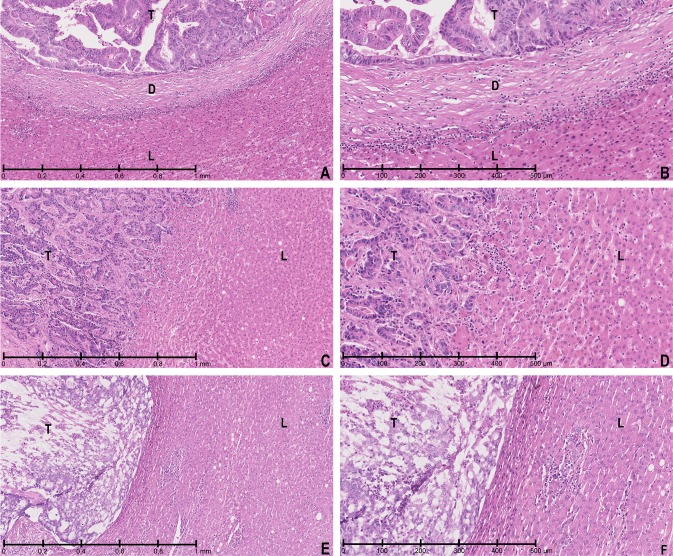
In patients with resectable colorectal liver metastases (CRLM), distinct histopathological growth patterns (HGPs) develop at the interface between the tumour and surrounding tissue. The desmoplastic (d) HGP is characterised by angiogenesis and a peripheral fibrotic rim, whereas non-angiogenic HGPs co-opt endogenous sinusoidal hepatic vasculature. Evidence from previous studies has suggested that patients with dHGP in their CRLM have improved prognosis as compared to patients with non-desmoplastic HGPs. However, these studies were relatively small and applied arbitrary cut-off values for the determination of the predominant HGP. We have now investigated the prognostic effect of dHGP in a large cohort of patients with CRLM resected either with or without neoadjuvant chemotherapy.
All consecutive patients undergoing a first partial hepatectomy for CRLM between 2000 and 2015 at a tertiary referral centre were considered for inclusion. HGPs were assessed in archival H&E stained slides according to recently published international consensus guidelines. The dHGP was defined as desmoplastic growth being present in 100% of the interface between the tumour and surrounding liver.
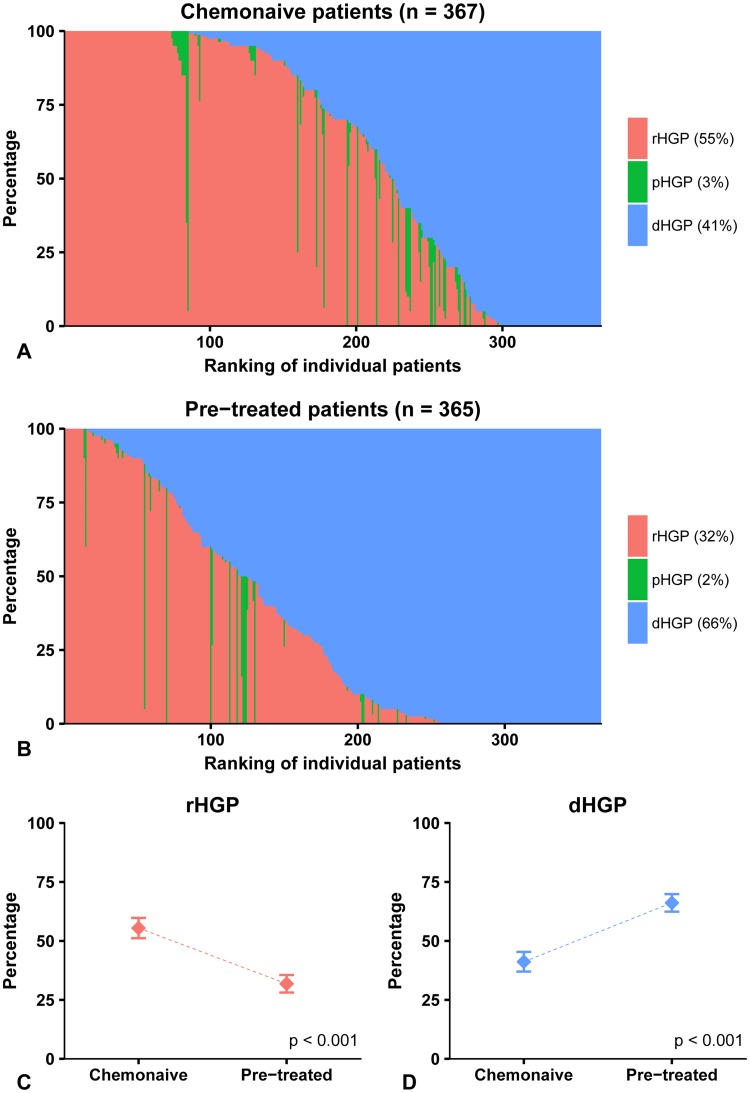
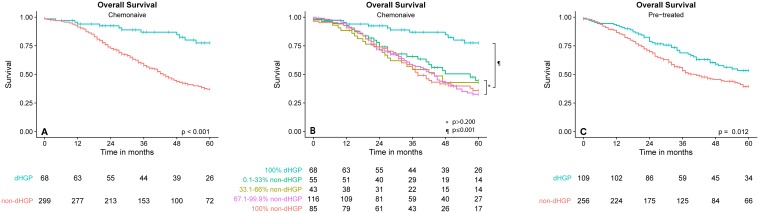
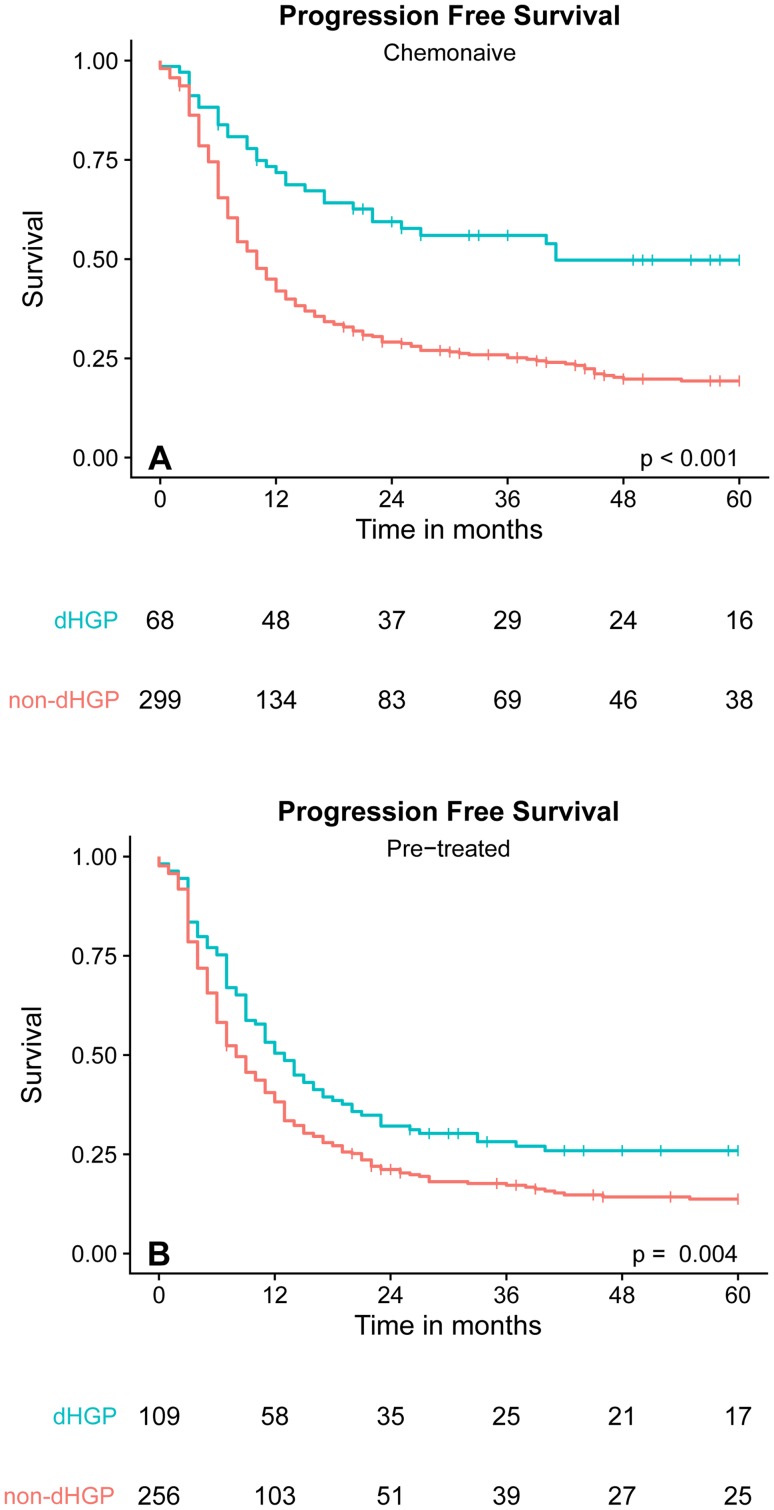
In total, HGPs in CRLMs from 732 patients were assessed. In the chemo-naive patient cohort (n = 367), the dHGP was present in 19% (n = 68) and the non-dHGP was present in 81% (n = 299) of patients. This dHGP subgroup was independently associated with good overall survival (OS) (HR: 0.39, p < 0.001) and progression-free survival (PFS) (HR: 0.54, p = 0.001). All patients with any CRLM with a non-dHGP had significantly reduced OS compared to those patients with 100% dHGP, regardless of the proportion of non-dHGP (all p values ≤ 0.001). In the neoadjuvantly treated patient cohort (n = 365), more patients were found to express dHGP (n = 109, 30%) (adjusted odds ratio: 2.71, p < 0.001). On univariable analysis, dHGP was associated with better OS (HR 0.66, p = 0.009) and PFS (HR 0.67, p = 0.002). However, after correction for confounding by means of multivariable analysis no significant association of dHGP with OS (HR 0.92, p = 0.623) or PFS (HR 0.76, p = 0.065) was seen.
The current study demonstrates that the angiogenic dHGP in CRLM resected from chemo-naive patients acts as a strong, positive prognostic marker, unmatched by any other prognosticator. This observation warrants the evaluation of the clinical utility of HGPs in prospective clinical trials.
在可切除结直肠癌肝转移(CRLM)患者中,肿瘤与周围组织交界处会出现不同的组织病理学生长模式(HGPs)。促血管生成的(d)HGP 的特征是血管生成和外围纤维状边缘,而非血管生成的 HGPs 则利用内源性肝窦状血管系统。来自先前研究的证据表明,与非促血管生成 HGPs 患者相比,dHGP 患者的 CRLM 预后更好。然而,这些研究规模相对较小,并且对确定主要 HGP 应用了任意的截止值。我们现在在接受新辅助化疗或未接受新辅助化疗的 CRLM 患者的大型队列中研究了 dHGP 的预后作用。
考虑纳入 2000 年至 2015 年期间在三级转诊中心接受首次部分肝切除术治疗的所有连续 CRLM 患者。根据最近发表的国际共识指南,在存档的 H&E 染色切片中评估 HGPs。dHGP 定义为肿瘤与周围肝脏之间的界面存在 100%的促血管生成生长。
总共评估了 732 例 CRLM 的 HGPs。在未接受化疗的患者队列(n=367)中,dHGP 存在于 19%(n=68)的患者中,非 dHGP 存在于 81%(n=299)的患者中。该 dHGP 亚组与良好的总生存(OS)(HR:0.39,p<0.001)和无进展生存(PFS)(HR:0.54,p=0.001)独立相关。所有非 100% dHGP 的 CRLM 患者的 OS 均明显低于 100% dHGP 患者,无论非 dHGP 的比例如何(所有 p 值均≤0.001)。在接受新辅助治疗的患者队列(n=365)中,更多的患者表现出 dHGP(n=109,30%)(调整优势比:2.71,p<0.001)。单变量分析显示,dHGP 与更好的 OS(HR 0.66,p=0.009)和 PFS(HR 0.67,p=0.002)相关。然而,在通过多变量分析校正混杂因素后,dHGP 与 OS(HR 0.92,p=0.623)或 PFS(HR 0.76,p=0.065)无显著关联。
目前的研究表明,促血管生成的 dHGP 在新辅助化疗的 CRLM 中是一种强大的、积极的预后标志物,没有其他预后标志物能与之媲美。这一观察结果需要在前瞻性临床试验中评估 HGPs 的临床实用性。