Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, Ohio.
Division of Critical Care Medicine, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio.
JAMA Netw Open. 2018 Sep 7;1(5):e182136. doi: 10.1001/jamanetworkopen.2018.2136.
New US health care payment models have increasingly incentivized health care systems to promote health and reduce health care spending at the population level, with Medicare beneficiaries representing one of the largest populations affected by new payment models. Identifying novel strategies to promote health and reduce health care spending is necessary.
To assess whether the overall well-being of a population is associated with health care spending for people 65 years of age or older.
DESIGN, SETTING, AND PARTICIPANTS: This US national, population-based cross-sectional study examined the association between county well-being and Medicare fee-for-service (FFS) spending. Population well-being, a holistic assessment of the overall health of the population comprising interrelated domains, including physical, mental, and social health, as measured by the Gallup-Sharecare Well-Being Index (2010), was linked to the mean spending per Medicare FFS beneficiary (2010) and county characteristics data for all US counties assessed. The data were adjusted for prevalence of 4 low-variation conditions (hip fracture, stroke, colorectal cancer, and acute myocardial infarction) and regional penetration of Medicare Advantage. Data analyses were conducted October 13, 2016, to October 31, 2017.
Mean spending per Medicare FFS beneficiary per county.
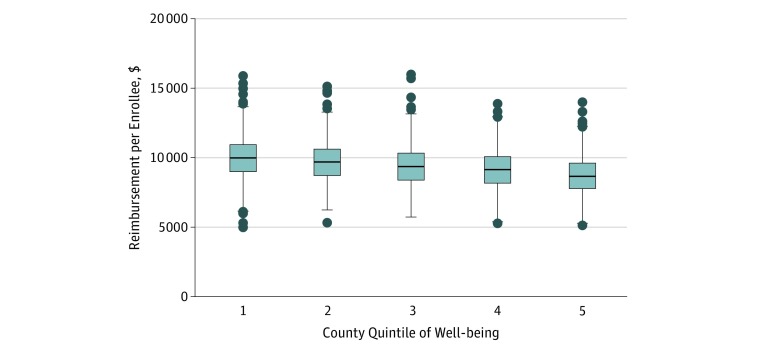
In total, 2998 counties were assessed using county-level mean values, with 4 to 7317 participants (mean [SD] number of participants, 755 [1220]) per county. The mean (SD) values of the demographic characteristics of the participants were 50.8% (1.3%) female, 74.9% (16.5%) white, 12.1% (13.0%) black, 4.0% (5.3%) Asian, and 13.7% (14.8%) Hispanic with a mean (SD) of the median county age of 38.2 (4.4) years. Medicare spent a mean (SE) of $992 ($110) less per Medicare FFS beneficiary in counties in the highest quintile of well-being compared with counties in the lowest well-being quintile. This inverse association persisted after accounting for key population characteristics such as median household income and contextual factors such as urbanicity and health care system capacity. Medicare spent a mean (SE) of $1233 ($104) less per Medicare FFS beneficiary in counties with the greatest access to basic needs than in those with the lowest access.
In this US national study, the overall well-being of a geographically defined population was inversely associated with its health care spending for people 65 years and older. Identifying this association between well-being and health care spending at the population level may help to lay the foundation for further study to first illuminate the mechanisms underlying the association and to second study interventions aimed at creating greater well-being and lower health care spending at the population level.
新的美国医疗保健支付模式越来越激励医疗保健系统在人口层面促进健康和降低医疗保健支出,其中 Medicare 受益人是受新支付模式影响最大的人群之一。有必要确定促进健康和降低医疗保健支出的新策略。
评估人群的整体幸福感是否与 65 岁及以上人群的医疗保健支出有关。
设计、地点和参与者:本项美国全国性、基于人群的横断面研究,考察了县幸福感与 Medicare 按服务项目付费(FFS)支出之间的关系。人口幸福感是对人口整体健康状况的综合评估,包括身体、精神和社会健康等相互关联的领域,使用的是盖洛普-沙尔卡健康指数(2010 年)进行衡量,该指数与 Medicare FFS 受益人的平均支出(2010 年)以及所有接受评估的美国县的县特征数据相关联。数据根据 4 种低变异情况(髋部骨折、中风、结直肠癌和急性心肌梗死)的流行率和 Medicare Advantage 的区域渗透率进行了调整。数据分析于 2016 年 10 月 13 日至 2017 年 10 月 31 日进行。
每个县 Medicare FFS 受益人的平均支出。
共评估了 2998 个县,每个县的平均(SD)参与者人数为 4 至 7317 人(755 [1220])。参与者的人口特征的平均(SD)值为 50.8%(1.3%)为女性,74.9%(16.5%)为白人,12.1%(13.0%)为黑人,4.0%(5.3%)为亚洲人,13.7%(14.8%)为西班牙裔,中位数县年龄的平均(SD)为 38.2(4.4)岁。幸福感最高的县 Medicare FFS 受益人的人均支出比幸福感最低的县 Medicare FFS 受益人的人均支出低$992($110)。在考虑了家庭中位数收入等关键人口特征以及城市状况和医疗保健系统能力等背景因素后,这种反比关系仍然存在。 Medicare FFS 受益人的人均支出在基本需求获取程度最高的县比在获取程度最低的县低$1233($104)。
在这项美国全国性研究中,地理位置确定的人群的整体幸福感与 65 岁及以上人群的医疗保健支出呈负相关。确定幸福感和人口健康支出之间的这种关联,可能有助于为进一步研究奠定基础,首先阐明关联背后的机制,其次研究旨在提高人口幸福感和降低健康支出的干预措施。