Singapore Institute for Clinical Sciences, Agency for Science, Technology and Research, Singapore, Singapore.
Division of Chronic Disease Research Across the Lifecourse, Department of Population Medicine, Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, Massachusetts.
JAMA Netw Open. 2018 Sep 7;1(5):e182460. doi: 10.1001/jamanetworkopen.2018.2460.
The American Academy of Pediatrics currently recommends weight for length (WFL) for assessment of weight status in children younger than 2 years but body mass index (BMI) for children older than 2 years. However, the clinical implications of using WFL vs BMI in children younger than 2 years as an indicator of future health outcomes remains understudied.
To compare associations of overweight based on WFL vs BMI in children younger than 2 years with cardiometabolic outcomes during early adolescence.
DESIGN, SETTING, AND PARTICIPANTS: This prospective study of birth cohorts in the United States (Project Viva) and Belarus (Promotion of Breastfeeding Intervention Trial [PROBIT]) performed from June 1, 1996, to November 31, 2002, included 13 666 children younger than 2 years.
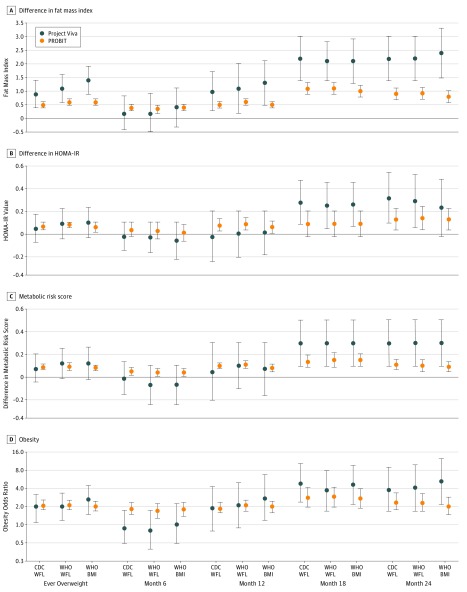
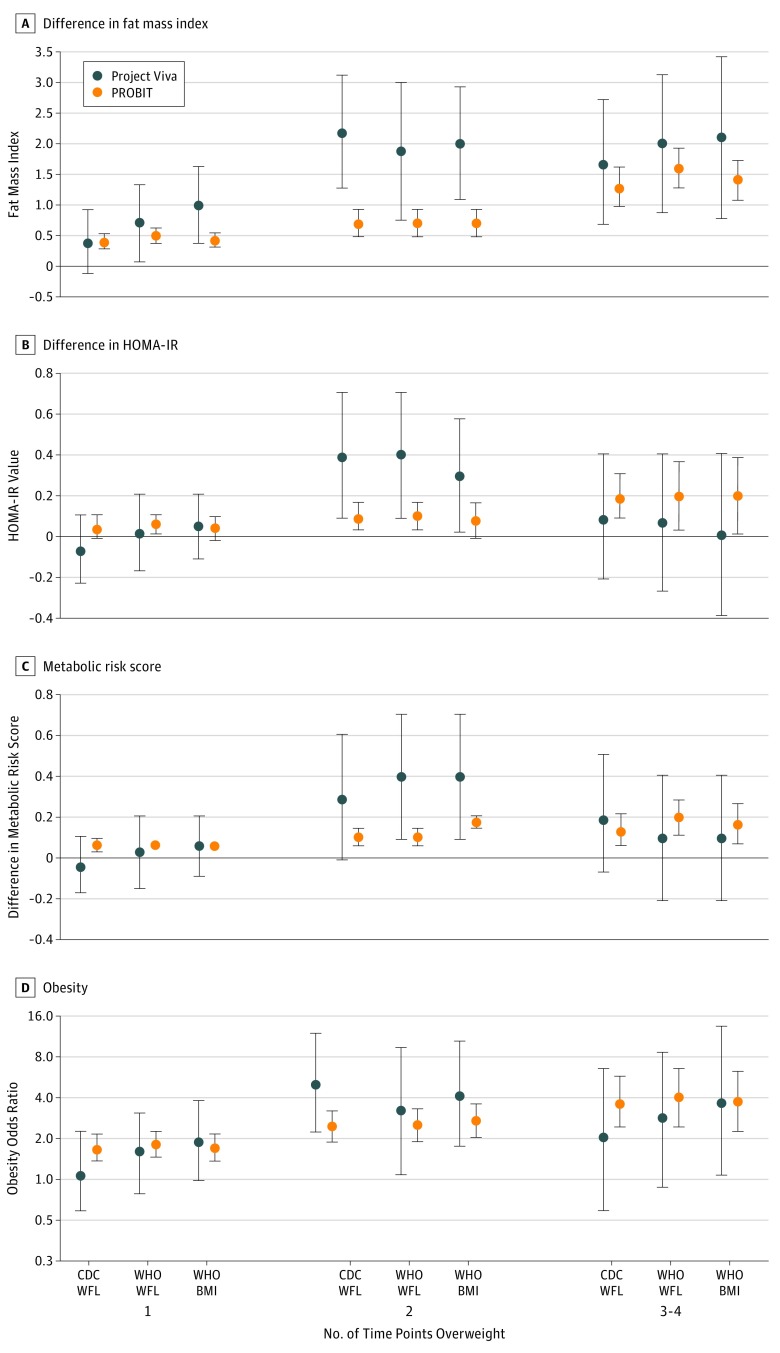
Overweight defined as Centers for Disease Control and Prevention (CDC) WFL in the 95th percentile or greater, World Health Organization (WHO) WFL in the 97.7th percentile or greater, or WHO BMI in the 97.7th percentile or greater at 6, 12, 18, or 24 months of age.
Primary outcomes were fat mass index, insulin resistance, metabolic risk score, and obesity during early adolescence. Secondary outcomes were height and BMI z scores, sum of skinfolds, waist circumference, and systolic blood pressure during early adolescence.
The study included 919 children (mean [SD] age, 12.9 [0.9] years; 460 [50.1%] male; and 598 [65.1%] white) from Project Viva and 12 747 children (mean [SD] age, 11.5 [0.5] years; 6204 [48.7%] male; and 12 747 [100%] white) from PROBIT. During 6 to 24 months of age, in Project Viva, 206 children (22.4%) were overweight at any of the 4 times points according to the CDC WFL, 160 (17.4%) according to WHO WFL, and 161 (17.5%) according to WHO BMI cut points. In PROBIT, 3715 children (29.1%) were overweight at any of the 4 time points according to the CDC WFL, 3069 (24.1%) according to WHO WFL, and 3125 (24.5%) according to WHO BMI cut points. After maternal and child characteristics were adjusted for, being ever overweight (vs never overweight) during 6 to 24 months of age was associated with higher likelihood of adverse cardiometabolic risk markers during early adolescence, but associations did not differ substantially across WFL and BMI cut points in either cohort. For example, for fat mass index in Project Viva, β = 0.9 (95% CI, 0.5-1.4) for the CDC WFL, β = 1.1 (95% CI, 0.6-1.6) for WHO WFL, and β = 1.4 (95% CI, 0.9-1.9) for WHO BMI. For PROBIT, β = 0.5 (95% CI, 0.4-0.6) for the CDC WFL, β = 0.6 (95% CI, 0.5-0.7) for WHO WFL, and β = 0.6 (95% CI, 0.5-0.6) for WHO BMI. Neither growth metric in infancy was superior over the others based on F statistics (Project Viva: 17.1-17.8; PROBIT: 87.1-88.7). Findings were similar for insulin resistance, metabolic risk score, obesity, and secondary outcomes.
Choice of WFL vs BMI to define overweight during the first 2 years of life may not greatly affect the association with cardiometabolic outcomes during early adolescence. The findings appear to have important implications for investigators seeking to use BMI as a growth metric for epidemiologic research and for practitioners monitoring the weight status of children younger than 2 years.
重要性:美国儿科学会目前建议使用体重长度(WFL)来评估 2 岁以下儿童的体重状况,但建议使用身体质量指数(BMI)来评估 2 岁以上儿童的体重状况。然而,WFL 与 BMI 作为 2 岁以下儿童未来健康结果的指标的临床意义仍有待研究。
目的:比较在 2 岁以下儿童中,超重的体重长度(WFL)与 BMI 与青少年早期的心血管代谢结局之间的相关性。
设计、设置和参与者:这项在美国(Viva 项目)和白俄罗斯(母乳喂养促进干预试验 [PROBIT])进行的出生队列前瞻性研究,于 1996 年 6 月 1 日至 2002 年 11 月 31 日进行,纳入了 13666 名 2 岁以下儿童。
主要暴露:超重定义为:根据疾病控制与预防中心(CDC)的 WFL,超过第 95 百分位数;或根据世界卫生组织(WHO)的 WFL,超过第 97.7 百分位数;或根据 WHO 的 BMI,超过第 97.7 百分位数,在 6、12、18 或 24 个月时测量。
主要结果和测量:主要结果是青少年早期的脂肪量指数、胰岛素抵抗、代谢风险评分和肥胖。次要结果是青少年早期的身高和 BMI 得分、皮褶厚度总和、腰围和收缩压。
结果:该研究纳入了来自 Viva 项目的 919 名儿童(平均[SD]年龄,12.9[0.9]岁;460[50.1%]为男性;598[65.1%]为白人)和 PROBIT 的 12747 名儿童(平均[SD]年龄,11.5[0.5]岁;6204[48.7%]为男性;12747[100%]为白人)。在 6 至 24 个月时,Viva 项目中有 206 名儿童(22.4%)在任何 4 个时间点根据 CDC 的 WFL 超重,160 名(17.4%)根据世卫组织的 WFL 超重,161 名(17.5%)根据世卫组织的 BMI 切点超重。在 PROBIT 中,有 3715 名儿童(29.1%)在任何 4 个时间点根据 CDC 的 WFL 超重,3069 名(24.1%)根据世卫组织的 WFL 超重,3125 名(24.5%)根据世卫组织的 BMI 切点超重。在调整了母婴特征后,在 6 至 24 个月时超重(与从不超重相比)与青少年早期心血管代谢风险标志物的发生几率增加有关,但在两个队列中,WFL 和 BMI 切点之间的关联并没有显著差异。例如,在 Viva 项目中,脂肪量指数的β值为 0.9(95%CI,0.5-1.4),为 CDC 的 WFL;β值为 1.1(95%CI,0.6-1.6),为世卫组织的 WFL;β值为 1.4(95%CI,0.9-1.9),为世卫组织的 BMI。对于 PROBIT,β值为 0.5(95%CI,0.4-0.6),为 CDC 的 WFL;β值为 0.6(95%CI,0.5-0.7),为世卫组织的 WFL;β值为 0.6(95%CI,0.5-0.6),为世卫组织的 BMI。基于 F 统计量(Viva 项目:17.1-17.8;PROBIT:87.1-88.7),这两个生长指标在婴儿期都没有优于其他指标。胰岛素抵抗、代谢风险评分、肥胖和次要结果的发现也相似。
结论和相关性:在生命的头 2 年中,使用 WFL 还是 BMI 来定义超重,可能不会对青少年早期的心血管代谢结果产生重大影响。这一发现对研究人员使用 BMI 作为流行病学研究的生长指标以及对监测 2 岁以下儿童体重状况的从业者具有重要意义。