Department of Surgery and Cancer, Imperial College London, St Mary's Hospital, Level 10, Praed Street, London, UK.
Department of General Surgery, Yeovil District Hospital NHS Foundation Trust, Higher Kingston, Yeovil, UK.
Surg Endosc. 2019 Oct;33(10):3370-3383. doi: 10.1007/s00464-018-06630-9. Epub 2019 Jan 17.
The role of laparoscopy in rectal cancer has been questioned. 3D laparoscopic systems are suggested to aid optimal surgical performance but have not been evaluated in advanced procedures. We hypothesised that stereoscopic imaging could improve the performance of laparoscopic total mesorectal excision (TME).
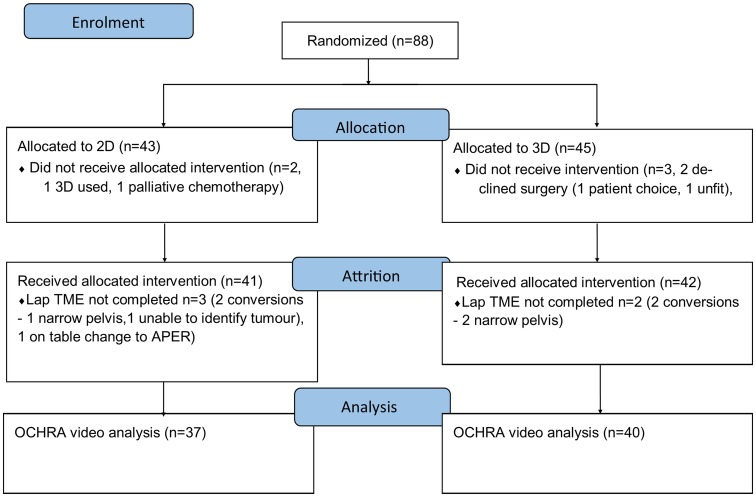
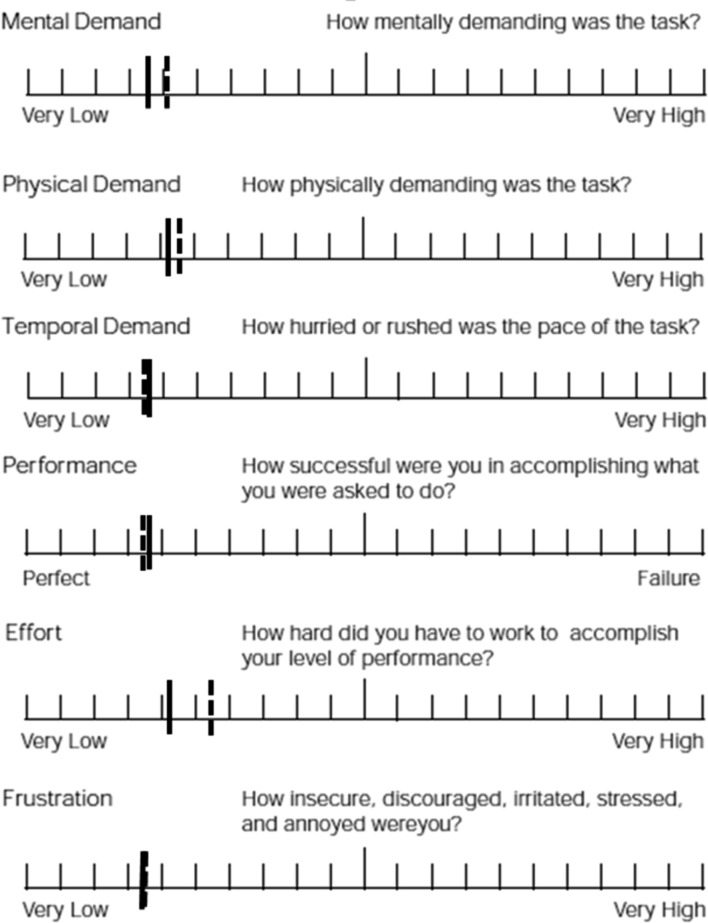
A multicentre developmental randomised controlled trial comparing 2D and 3D laparoscopic TME was performed (ISRCTN59485808). Trial surgeons were colorectal consultants that had completed their TME proficiency curve and underwent stereoscopic visual testing. Patients requiring elective laparoscopic TME with curative intent were centrally randomised (1:1) to 2D or 3D using Karl Storz IMAGE1 S D3-Link™ and 10-mm TIPCAM®1S 3D passive polarising laparoscopic systems. Outcomes were enacted adverse events as assessed by the observational clinical human reliability analysis technique, intraoperative data, 30-day patient outcomes, histopathological specimen assessment and surgeon cognitive load.
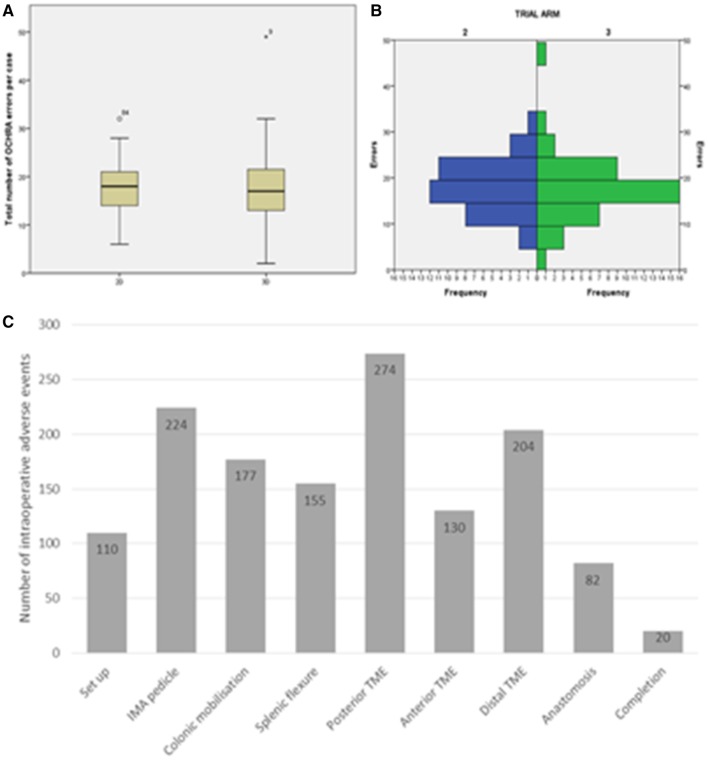
88 patients were included. There were no differences in patient or tumour demographics, surgeon stereopsis, case difficulty, cognitive load, operative time, blood loss or conversion between the trial arms. 1377 intraoperative adverse events were identified (median 18 per case, IQR 14-21, range 2-49) with no differences seen between the 2D and 3D arms (18 (95% CI 17-21) vs. 17 (95% CI 16-19), p = 0.437). 3D laparoscopy had non-significantly higher mesorectal fascial plane resections (94 vs. 77%, p = 0.059; OR 0.23 (95% CI 0.05-1.16)) but equal lymph node yield and circumferential margin distance and involvement. 30-day morbidity, anastomotic leak, re-operation, length of stay and readmission rates were equal between the 2D and 3D arms.
Feasibility of performing multicentre 3D laparoscopic multicentre trials of specialist performed complex procedures is shown. 3D imaging did not alter the number of intraoperative adverse events; however, a potential improvement in mesorectal specimen quality was observed and should form the focus of future 3D laparoscopic TME trials.
腹腔镜在直肠癌中的作用受到质疑。三维腹腔镜系统被认为有助于实现最佳手术效果,但尚未在先进手术中进行评估。我们假设立体成像可以提高腹腔镜全直肠系膜切除术(TME)的效果。
进行了一项比较二维和三维腹腔镜 TME 的多中心发展性随机对照试验(ISRCTN59485808)。试验外科医生是已完成 TME 熟练曲线并接受立体视觉测试的结直肠顾问。需要进行根治性腹腔镜 TME 的择期患者使用 Karl Storz IMAGE1 S D3-Link™ 和 10-mm TIPCAM®1S 3D 被动偏振腹腔镜系统进行中央随机分组(1:1)。结局为观察性临床人体可靠性分析技术评估的不良事件,术中数据,30 天患者结局,组织病理学标本评估和外科医生认知负荷。
纳入 88 例患者。两组患者和肿瘤人口统计学,外科医生立体视,手术难度,认知负荷,手术时间,出血量或转化率均无差异。在试验臂之间未发现 2D 和 3D 之间的差异(18(95%CI 17-21)与 17(95%CI 16-19),p = 0.437)。发现 1377 例术中不良事件(中位数为每例 18 例,IQR 为 14-21,范围为 2-49)。3D 腹腔镜具有更高的直肠筋膜平面切除率(94%与 77%,p = 0.059;OR 0.23(95%CI 0.05-1.16)),但淋巴结产量,环形切缘距离和受累程度相等。2D 和 3D 臂之间 30 天发病率,吻合口漏,再次手术,住院时间和再入院率相等。
显示了进行多中心 3D 腹腔镜多中心试验的可行性,这些试验涉及专家进行的复杂手术。3D 成像并未改变术中不良事件的数量;但是,观察到直肠标本质量的潜在改善,应成为未来 3D 腹腔镜 TME 试验的重点。