Wojtaszek Ewa, Grzejszczak Agnieszka, Grygiel Katarzyna, Małyszko Jolanta, Matuszkiewicz-Rowińska Joanna
Department of Nephrology, Dialysis and Internal Medicine, Warsaw Medical University, Warsaw, Poland.
Department of General, Vascular and Transplant Surgery, Warsaw Medical University, Warsaw, Poland.
Front Physiol. 2019 Jan 4;9:1830. doi: 10.3389/fphys.2018.01830. eCollection 2018.
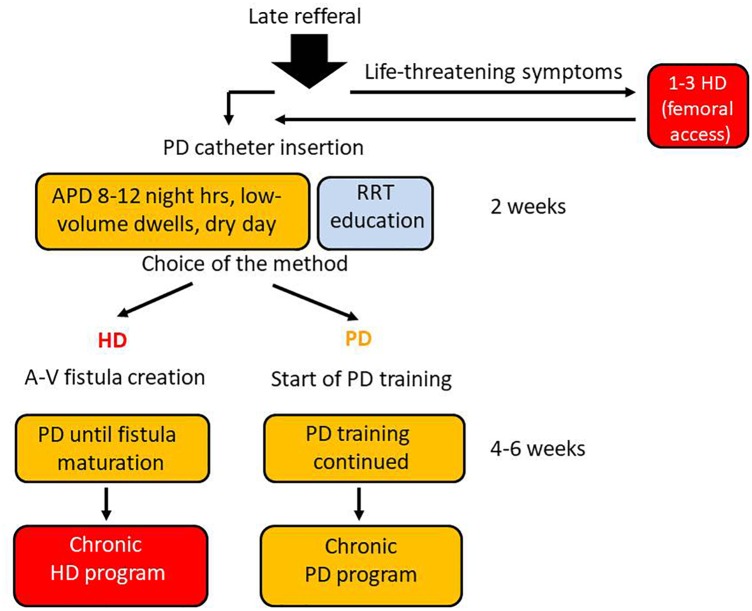
The peritoneal dialysis (PD) urgent-start pathway, without typical 2-week break-in period, was meant for late-referral patients able and prone to join PD-first program, with its main advantages such as: keeping the vascular system intact, preserving their residual renal function and retaining life-style flexibility. We compared the short- and long-term outcomes of consecutive 35 patients after urgent- and 94 patients after the planned start of PD as the first choice. The study included all incident end-stage renal disease patients starting PD program between January 2005 and December 2015, classified into two groups: those with urgent (unplanned) and those with elective (planned) start. Urgent PD was initiated as an overnight automatic procedure (APD) with dwell volume gradually increased, and after 2-3 weeks, target PD method was established. The mean time between catheter implantation and PD start was 3.5 ± 2.3 in urgent and 16.2 ± 1.7 days in planned-start groups ( < 0.00001). 51% of the patients in the urgent-start group required PD during first 48 h after catheter insertion. Mean follow-up of 17.6 ± 11.09 months (median: 19.0) was in the urgent-start group and 28.6 ± 26.6 months (median: 19.5) in the planned-start group. The early mechanical complications were observed more often in the urgent-start group (29 vs. 4%, = 0.00005). The only significant predictors of early mechanical complications were serum albumin ( = 0.02) and time between the catheter insertion and PD start. The first year patient survival and technique survival censored for death and kidney transplantation were not significantly different between groups. In Cox proportional analysis the independent risk factors for patient survival as well as for method and patient survival appeared Charlson Comorbidity Index CCI (HR 1.4; = 0.01 and 1.24; = 0.02) and time from catheter implantation to PD start with HR 5.11; = 0.03 and 4.29; = 0.04 for <2 days, while time >14 days lost its predictive value ( = 0.07). Peritoneal dialysis may be a feasible and safe alternative to HD in patients who need to start dialysis urgently without established dialysis access, with an acceptable complications rates, as well as patient and technique survival.
腹膜透析(PD)紧急启动途径,没有典型的2周磨合期,适用于有能力且倾向于加入优先选择PD方案的转诊延迟患者,其主要优点包括:保持血管系统完整、保留残余肾功能以及保持生活方式的灵活性。我们比较了35例紧急开始PD的患者和94例计划开始PD的患者作为首选治疗后的短期和长期结局。该研究纳入了2005年1月至2015年12月期间开始PD治疗的所有新发终末期肾病患者,分为两组:紧急(非计划)开始组和择期(计划)开始组。紧急PD作为夜间自动腹膜透析(APD)开始,留腹容量逐渐增加,2 - 3周后确定目标PD方法。紧急开始组导管植入与PD开始之间的平均时间为3.5±2.3天,计划开始组为16.2±1.7天(P<0.00001)。紧急开始组51%的患者在导管插入后的前48小时内需要进行PD。紧急开始组的平均随访时间为17.6±11.09个月(中位数:19.0个月),计划开始组为28.6±26.6个月(中位数:19.5个月)。紧急开始组早期机械并发症的发生率更高(29%对4%,P = 0.00005)。早期机械并发症的唯一显著预测因素是血清白蛋白(P = 0.02)以及导管插入与PD开始之间的时间。两组之间第一年校正死亡和肾移植后的患者生存率和技术生存率没有显著差异。在Cox比例分析中,患者生存以及方法和患者生存的独立危险因素为Charlson合并症指数(CCI)(风险比[HR] 1.4;P = 0.01和1.24;P = 0.02)以及从导管植入到PD开始的时间,开始时间<2天的HR为5.11;P = 0.03和4.29;P = 0.04,而开始时间>14天则失去其预测价值(P = 0.07)。对于急需开始透析但尚未建立透析通路的患者,腹膜透析可能是血液透析的一种可行且安全的替代方法,并发症发生率可接受,患者生存率和技术生存率也较好。