Departments of Anaesthesiology, Physiology, and Cardiothoracic Surgery, Amsterdam UMC, VU University, Amsterdam Cardiovascular Sciences, Amsterdam, the Netherlands.
Department of Intensive Care Medicine, Research VUmc Intensive Care (REVIVE), Amsterdam UMC, VU University, Amsterdam Infection and Immunity Institute, Amsterdam, the Netherlands.
Anaesthesia. 2019 May;74(5):609-618. doi: 10.1111/anae.14577. Epub 2019 Jan 27.
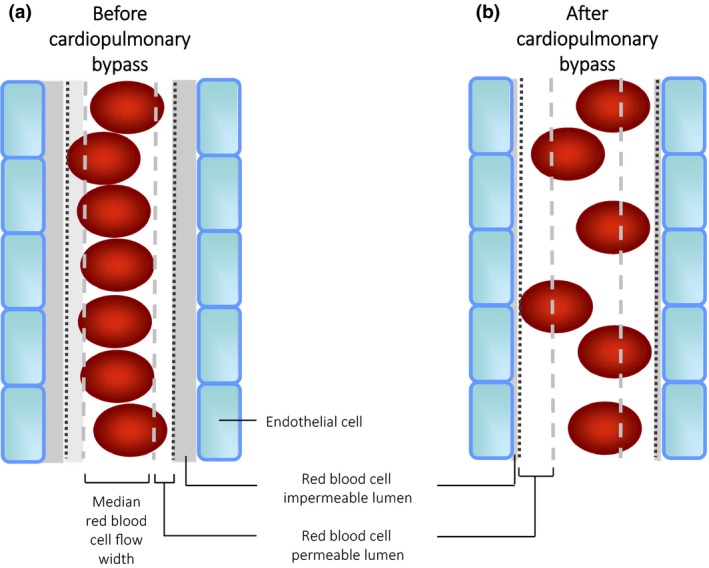
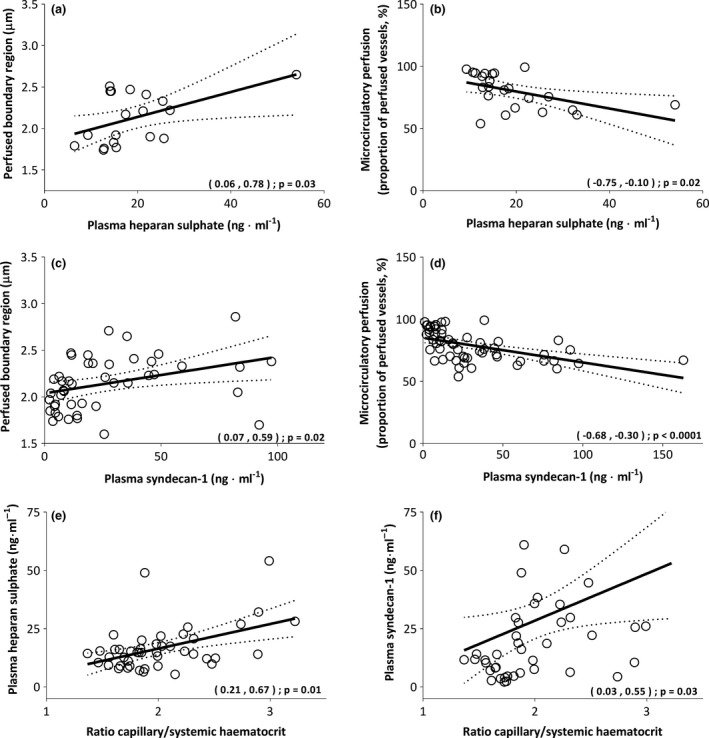
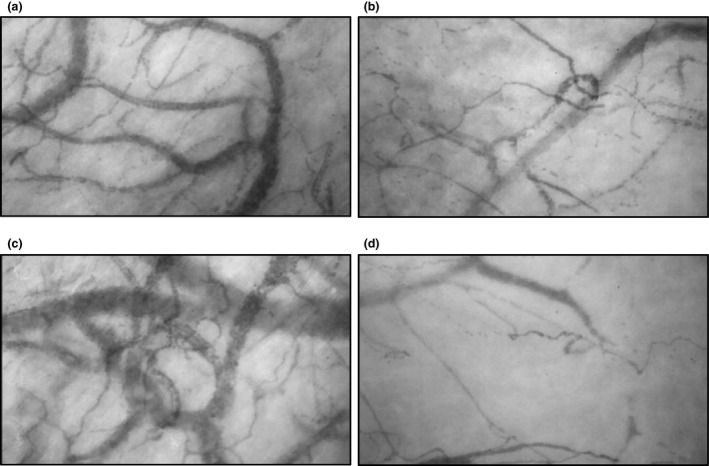
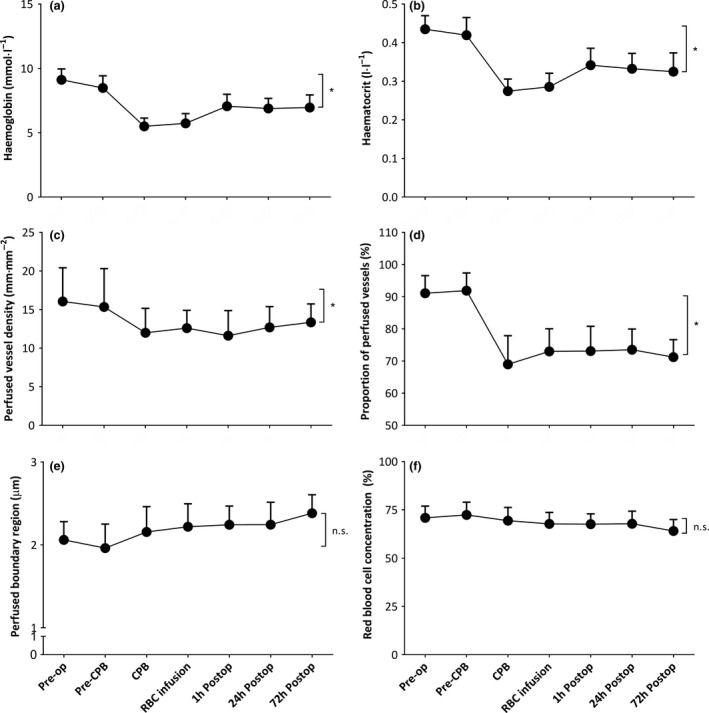
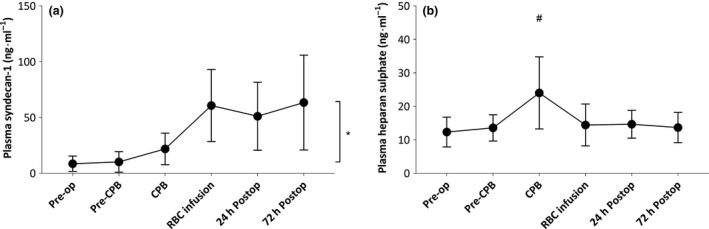
We investigated microcirculatory perfusion disturbances following cardiopulmonary bypass in the early postoperative period and whether the course of these disturbances mirrored restoration of endothelial glycocalyx integrity. We performed sublingual sidestream dark field imaging of the microcirculation during the first three postoperative days in patients who had undergone on-pump coronary artery bypass graft surgery. We calculated the perfused vessel density, proportion of perfused vessels and perfused boundary region. Plasma was obtained to measure heparan sulphate and syndecan-1 levels as glycocalyx shedding markers. We recruited 17 patients; the mean (SD) duration of non-pulsatile cardiopulmonary bypass was 103 (18) min, following which 491 (29) ml autologous blood was transfused through cell salvage. Cardiopulmonary bypass immediately decreased both microcirculatory perfused vessel density; 11 (3) vs. 16 (4) mm.mm , p = 0.052 and the proportion of perfused vessels; 92 (5) vs. 69 (9) %, p < 0.0001. The proportion of perfused vessels did not increase after transfusion of autologous salvaged blood following cardiopulmonary bypass; 72 (7) %, p = 0.19 or during the first three postoperative days; 71 (5) %, p < 0.0001. The perfused boundary region increased after cardiopulmonary bypass; 2.2 (0.3) vs. 1.9 (0.3) μm, p = 0.037 and during the first three postoperative days; 2.4 (0.3) vs. 1.9 (0.3) μm, p = 0.003. Increased plasma heparan sulphate levels were inversely associated with the proportion of perfused vessels during cardiopulmonary bypass; R = -0.49, p = 0.02. Plasma syndecan-1 levels were inversely associated with the proportion of perfused vessels during the entire study period; R = -0.51, p < 0.0001. Our study shows that cardiopulmonary bypass-induced acute microcirculatory perfusion disturbances persist in the first three postoperative days, and are associated with prolonged endothelial glycocalyx shedding. This suggests prolonged impairment and delayed recovery of both microcirculatory perfusion and function after on-pump cardiac surgery.
我们研究了体外循环后早期术后的微循环灌注障碍,以及这些障碍的发生过程是否与内皮糖萼完整性的恢复相吻合。我们对接受体外循环冠状动脉旁路移植术的患者在术后头 3 天进行舌下侧支暗场成像,以测量微循环灌注。我们计算了灌注血管密度、灌注血管比例和灌注边界区域。采集血浆以测量硫酸乙酰肝素和连接蛋白-1 水平作为糖萼脱落标志物。我们招募了 17 名患者;无搏动体外循环的平均(SD)持续时间为 103(18)min,随后通过细胞保存输注 491(29)ml 自体血。体外循环后立即降低了微血管灌注血管密度;11(3)vs. 16(4)mm.mm,p=0.052 和灌注血管比例;92(5)vs. 69(9)%,p<0.0001。体外循环后输注自体回收血后,灌注血管比例并未增加;72(7)%,p=0.19 或在术后头 3 天;71(5)%,p<0.0001。体外循环后灌注边界区域增加;2.2(0.3)vs. 1.9(0.3)μm,p=0.037 和术后头 3 天;2.4(0.3)vs. 1.9(0.3)μm,p=0.003。体外循环过程中肝素硫酸水平的升高与灌注血管比例呈负相关;R=-0.49,p=0.02。整个研究期间,血浆连接蛋白-1水平与灌注血管比例呈负相关;R=-0.51,p<0.0001。我们的研究表明,体外循环引起的急性微循环灌注障碍在术后头 3 天持续存在,并与内皮糖萼脱落延长有关。这表明体外循环心脏手术后,微循环灌注和功能的损伤持续时间延长,恢复时间延迟。