van Es René, van den Broek Hans T, van der Naald Mira, de Jong Leon, Nieuwenhuis Eliane R, Kraaijeveld Adriaan O, Doevendans Pieter A, Chamuleau Steven A J, van Slochteren Frebus J
Department of Cardiology, Division Heart and Lungs, University Medical Center Utrecht, PO Box 85500, 3508GA, Utrecht, The Netherlands.
MIRA Institute for Biomedical Engineering and Technical Medicine, University of Twente, Enschede, The Netherlands.
Int J Cardiovasc Imaging. 2019 Feb;35(2):225-235. doi: 10.1007/s10554-019-01541-9. Epub 2019 Jan 28.
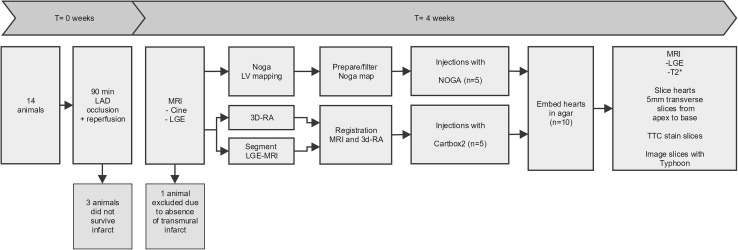
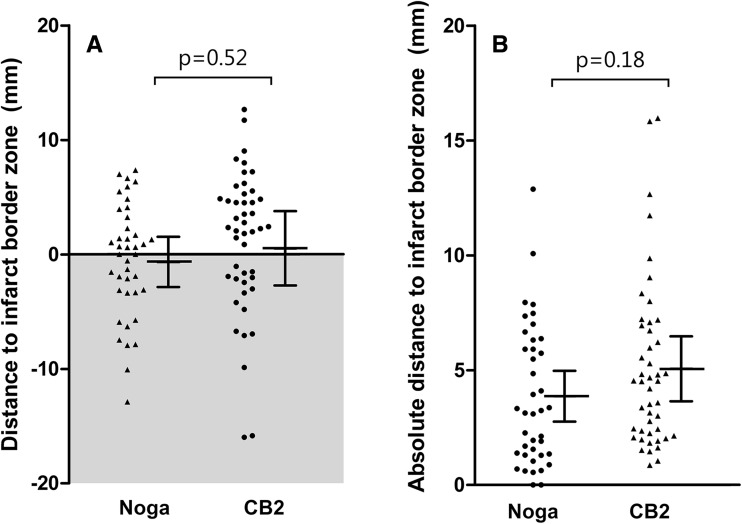
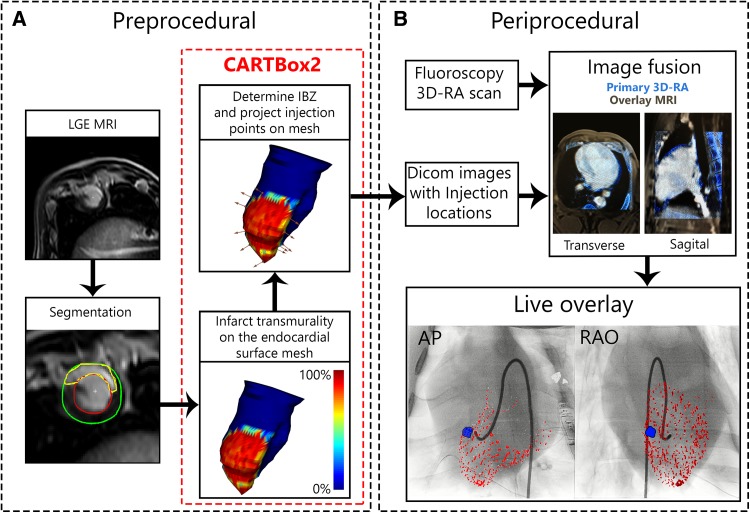
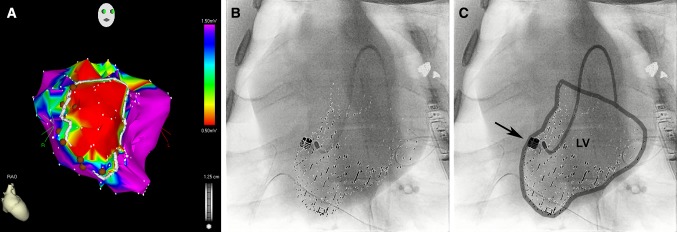
Comparison of the targeting accuracy of a new software method for MRI-fluoroscopy guided endomyocardial interventions with a clinically available 3D endocardial electromechanical mapping system. The new CARTBox2 software enables therapy target selection based on infarction transmurality and local myocardial wall thickness deduced from preoperative MRI scans. The selected targets are stored in standard DICOM datasets. Fusion of these datasets with live fluoroscopy enables real-time visualization of MRI defined targets during fluoroscopy guided interventions without the need for external hardware. In ten pigs (60-75 kg), late gadolinium enhanced (LGE) MRI scans were performed 4 weeks after a 90-min LAD occlusion. Subsequently, 10-16 targeted fluorescent biomaterial injections were delivered in the infarct border zone (IBZ) using either the NOGA 3D-mapping system or CARTBox2. The primary endpoint was the distance of the injections to the IBZ on histology. Secondary endpoints were total procedure time, fluoroscopy time and dose, and the number of ventricular arrhythmias. The average distance of the injections to the IBZ was similar for CARTBox2 (0.5 ± 3.2 mm) and NOGA (- 0.7 ± 2.2 mm; p = 0.52). Injection procedures with CARTBox2 and NOGA required 69 ± 12 and 60 ± 17 min, respectively (p = 0.36). The required endocardial mapping procedure with NOGA prior to injections, leads to a significantly longer total procedure time (p < 0.001) with NOGA. Fluoroscopy time with NOGA (18.7 ± 11.0 min) was significantly lower than with CARTBox2 (43.4 ± 6.5 min; p = 0.0003). Procedures with CARTBox2 show a trend towards less ventricular arrhythmias compared to NOGA. CARTBox2 is an accurate and fast software-only system to facilitate cardiac catheter therapy based on gold standard MRI imaging and live fluoroscopy.
一种用于磁共振成像-荧光透视引导的心内膜介入治疗的新软件方法与临床可用的三维心内膜机电标测系统的靶向准确性比较。新的CARTBox2软件能够根据术前磁共振成像扫描推断的梗死透壁性和局部心肌壁厚度来选择治疗靶点。所选靶点存储在标准的DICOM数据集中。将这些数据集与实时荧光透视融合,可在荧光透视引导介入过程中实时可视化磁共振成像定义的靶点,而无需外部硬件。对10头猪(60 - 75千克)在90分钟左前降支闭塞4周后进行延迟钆增强(LGE)磁共振成像扫描。随后,使用NOGA三维标测系统或CARTBox2在梗死边缘区(IBZ)进行10 - 16次靶向荧光生物材料注射。主要终点是组织学上注射点到IBZ的距离。次要终点包括总操作时间、荧光透视时间和剂量以及室性心律失常的数量。CARTBox2(0.5±3.2毫米)和NOGA(-0.7±2.2毫米;p = 0.52)的注射点到IBZ的平均距离相似。使用CARTBox2和NOGA进行注射操作分别需要69±12分钟和60±17分钟(p = 0.36)。使用NOGA在注射前进行的心内膜标测操作导致总操作时间显著更长(p < 0.001)。使用NOGA的荧光透视时间(18.7±11.0分钟)显著低于使用CARTBox2的时间(43.4±6.5分钟;p = 0.0003)。与NOGA相比,使用CARTBox2的操作显示出室性心律失常较少的趋势。CARTBox2是一种准确且快速的纯软件系统,可基于金标准磁共振成像和实时荧光透视促进心脏导管治疗。