Goldfarb Lucas, Duchemann Boris, Chouahnia Kader, Zelek Laurent, Soussan Michael
Department of Nuclear Medicine, Paris 13 University, APHP, Hôpital Avicenne, 125 rue de Stalingrad, 93000, Bobigny, France.
Department of Oncology, Paris 13 University, APHP, Hôpital Avicenne, Bobigny, France.
EJNMMI Res. 2019 Jan 29;9(1):8. doi: 10.1186/s13550-019-0473-1.
Immunotherapy represents a new therapeutic approach in non-small cell lung carcinoma (NSCLC) with the potential for prolonged benefits. Because of the systemic nature and heterogeneity of tumoral diseases, as well as the immune restoration process induced by immunotherapy, the assessment of therapeutic efficacy is challenging, and the role of FDG PET is not well established. We evaluated the potential of FDG PET to monitor NSCLC patients treated with a checkpoint inhibitor.
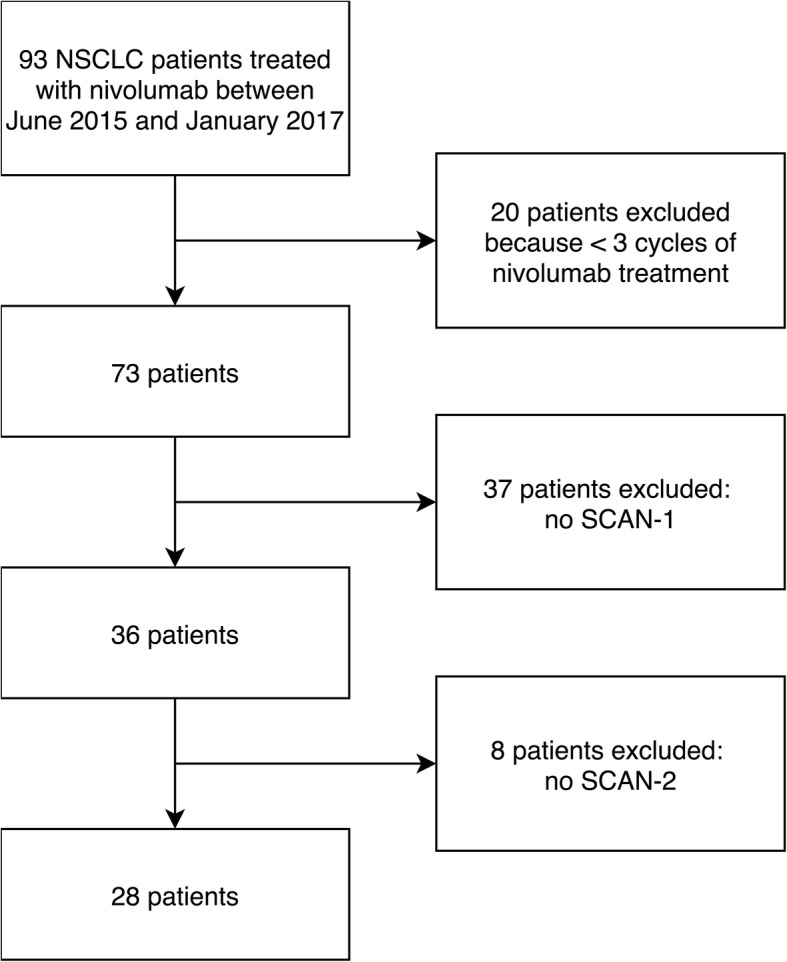
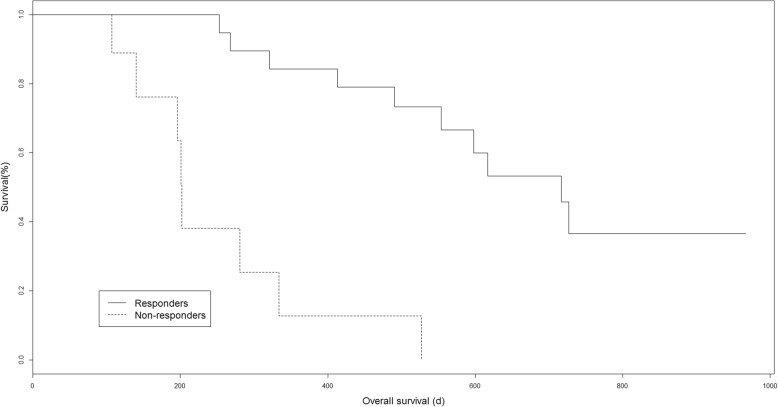
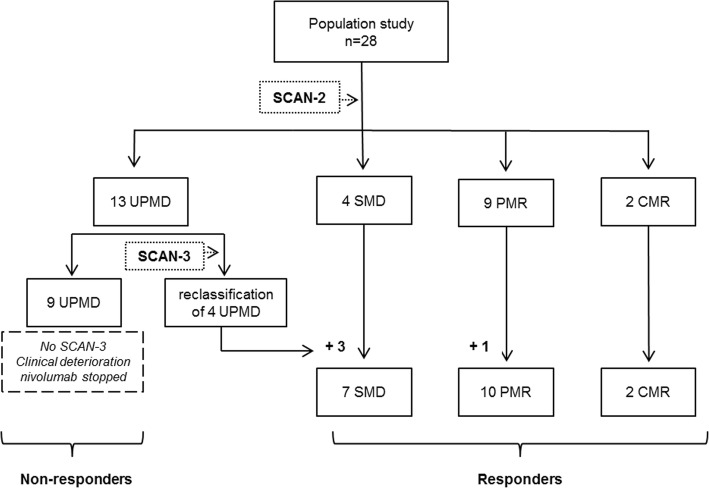
This was a retrospective analysis of 28 NSCLC patients treated with nivolumab, a programmed cell death 1 (PD-1) blocker. All patients underwent a PET scan before treatment (SCAN-1) and another scan 2 months later (SCAN-2). Disease progression was assessed by immune PET Response Criteria in Solid Tumors (iPERCIST), which was adapted from PERCIST; and the immune Response Evaluation Criteria in Solid Tumors (iRECIST). iPERCIST is a dual-time-point evaluation of "unconfirmed progressive metabolic disease" (UPMD) status at SCAN-2. UPMD at SCAN-2 was re-evaluated after 4 weeks with SCAN-3 to confirm PMD. Patients with complete/partial metabolic response (CMR or PMR) or stable metabolic disease (SMD) at SCAN-2 or -3 were considered responders. Patients with UPMD confirmed at SCAN-3 were considered non-responders. The Kaplan-Meier method was used to estimate survival. At SCAN-2, we found 9/28 cases of PMR, 4/28 cases of SMD, 2/28 cases of CMR, and 13/28 cases of UPMD. Four of the 13 UPMD patients were classified as responders at SCAN-3 (PMR n = 1, SMD n = 3). The remaining nine UPMD patients were classified as non-responders due to clinical degradation, and treatment was stopped. The median follow-up was 16.7 months [3.6-32.2]. Responders continued treatment for a mean of 10.7 months [3.8-26.3]. Overall survival was longer for responders than that for non-responders (19.9 vs. 3.6 months, log rank p = 0.0003). The 1-year survival rates were 94% for responders and 11% for non-responders. A comparison with iRECIST showed reclassification in 39% (11/28) of patients with relevant additional prognostic information.
iPERCIST dual-time-point evaluation might be a powerful tool for evaluating anti-PD-1-based immunotherapy, with the ability to identify patients who can benefit most from treatment. The prognostic value of iPERCIST criteria should be confirmed in large prospective multicentric studies.
免疫疗法是治疗非小细胞肺癌(NSCLC)的一种新方法,具有带来长期益处的潜力。由于肿瘤疾病的全身性和异质性,以及免疫疗法诱导的免疫恢复过程,治疗效果评估具有挑战性,且氟代脱氧葡萄糖正电子发射断层扫描(FDG PET)的作用尚未明确。我们评估了FDG PET监测接受检查点抑制剂治疗的NSCLC患者的潜力。
这是一项对28例接受纳武单抗(一种程序性细胞死亡蛋白1(PD-1)阻断剂)治疗的NSCLC患者的回顾性分析。所有患者在治疗前均接受了PET扫描(扫描1),并在2个月后进行了另一次扫描(扫描2)。通过实体瘤免疫PET反应标准(iPERCIST,改编自PERCIST)和实体瘤免疫反应评估标准(iRECIST)评估疾病进展。iPERCIST是对扫描2时“未确认的进行性代谢疾病”(UPMD)状态的双时间点评估。在4周后用扫描3对扫描2时的UPMD进行重新评估以确认进行性代谢疾病(PMD)。在扫描2或扫描3时具有完全/部分代谢反应(CMR或PMR)或稳定代谢疾病(SMD)的患者被视为反应者。在扫描3时确认有UPMD的患者被视为无反应者。采用Kaplan-Meier法估计生存率。在扫描2时,我们发现9/28例为PMR,4/28例为SMD,2/28例为CMR,13/28例为UPMD。13例UPMD患者中有4例在扫描3时被分类为反应者(PMR n = 1,SMD n = 3)。其余9例UPMD患者因临床病情恶化被分类为无反应者,并停止治疗。中位随访时间为16.7个月[3.6 - 32.2]。反应者继续治疗的平均时间为10.7个月[3.8 - 26.3]。反应者的总生存期长于无反应者(19.9个月对3.6个月,对数秩检验p = 0.0003)。反应者的1年生存率为94%,无反应者为11%。与iRECIST的比较显示,39%(11/28)的患者有相关的额外预后信息重新分类。
iPERCIST双时间点评估可能是评估基于抗PD-1免疫疗法的有力工具,能够识别最能从治疗中获益的患者。iPERCIST标准的预后价值应在大型前瞻性多中心研究中得到证实。