Department of Orthopedics, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China.
BMJ Open. 2019 Jan 28;9(1):e024350. doi: 10.1136/bmjopen-2018-024350.
This study aimed to compare the effects of intravenous, topical and combined routes of tranexamic acid (TXA) administration on blood loss and transfusion requirements in patients undergoing total knee arthroplasty (TKA) and total hip arthroplasty (THA).
This was a meta-analysis of randomised controlled trials (RCT) wherein the weighted mean difference (WMD) and relative risk (RR) were used for data synthesis applied in the random effects model. Stratified analyses based on the surgery type, region, intravenous and topical TXA dose and transfusion protocol were also conducted. The main outcomes included intraoperative and total blood loss volume, transfusion rate, low postoperative haemoglobin (Hb) level and postoperative Hb decline. However, the secondary outcomes included length of hospital stay (LOS) and/or occurrence of venous thromboembolism (VTE).
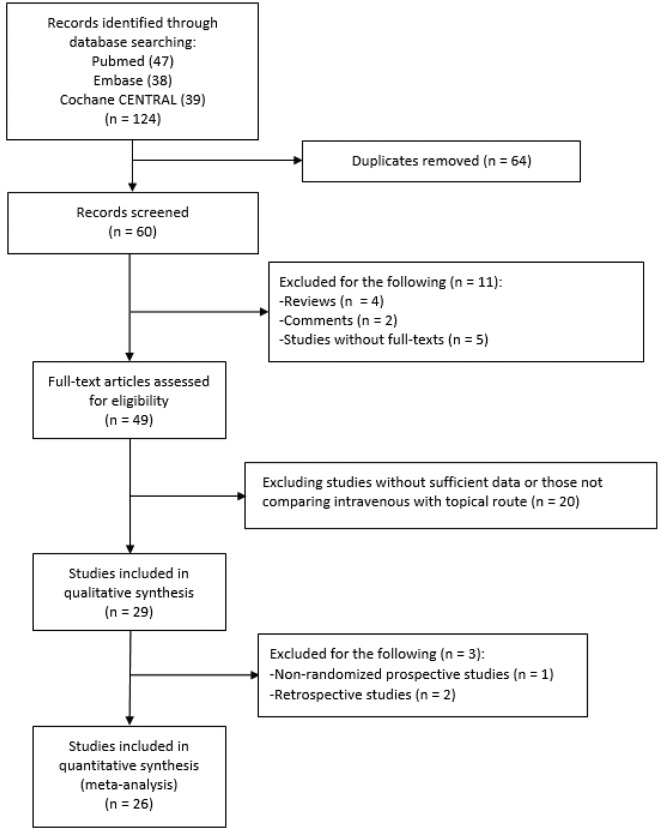
We searched the PubMed, Embase and Cochrane CENTRAL databases for RCTs that compared different routes of TXA administration.
Patients undergoing TKA or THA.
Intravenous, topical or combined intravenous and topical TXA.
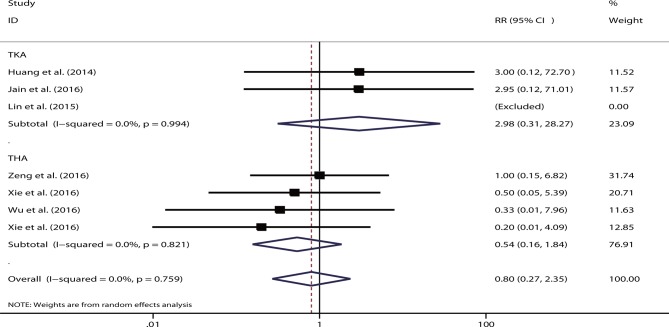
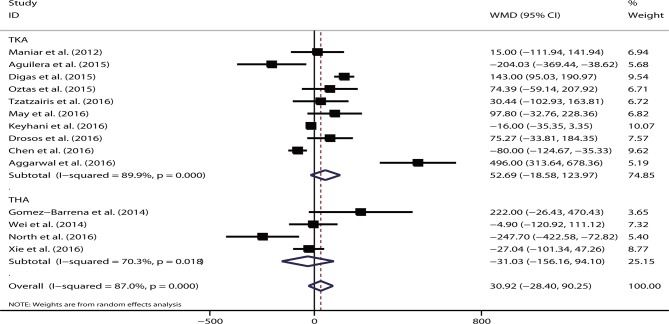
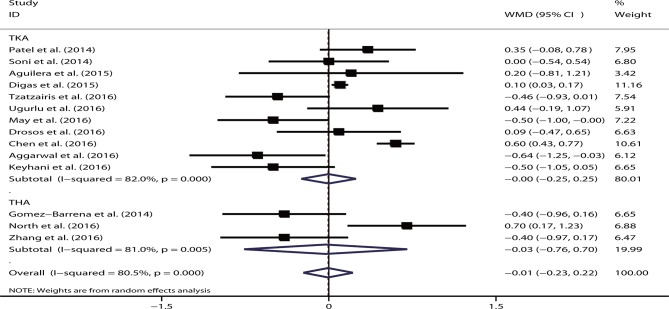
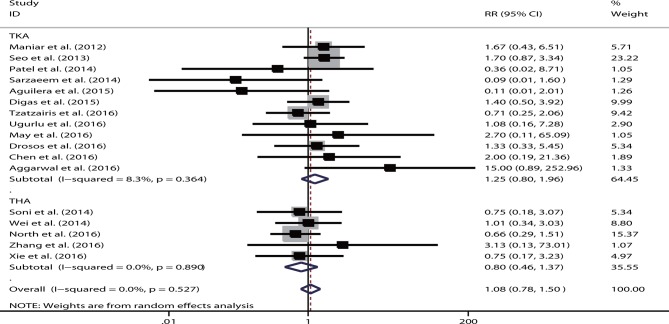
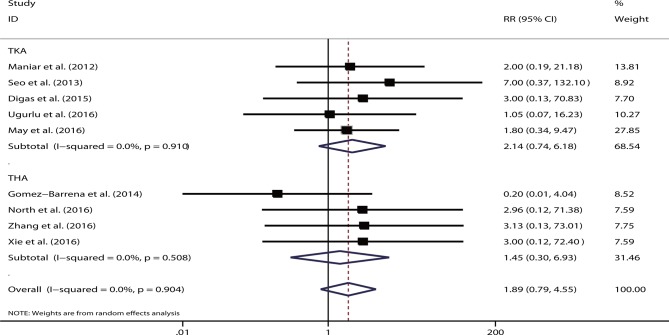
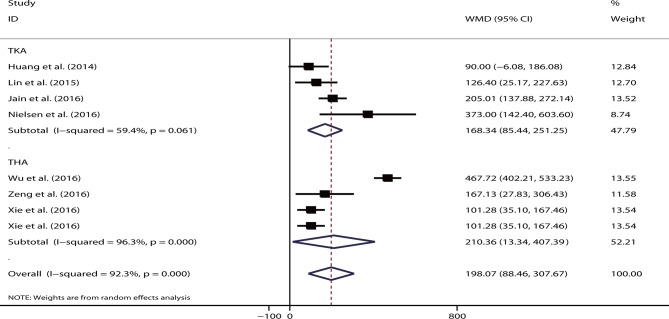
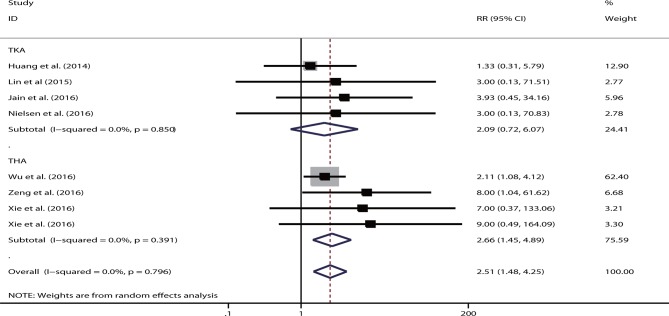
Twenty-six RCTs were selected, and the intravenous route did not differ substantially from the topical route with respect to the total blood loss volume (WMD=30.92, p=0.31), drain blood loss (WMD=-34.53, p=0.50), postoperative Hb levels (WMD=-0.01, p=0.96), Hb decline (WMD=-0.39, p=0.08), LOS (WMD=0.15, p=0.38), transfusion rate (RR=1.08, p=0.75) and VTE occurrence (RR=1.89, p=0.15). Compared with the combined-delivery group, the single-route group had significantly increased total blood loss volume (WMD=198.07, p<0.05), greater Hb decline (WMD=0.56, p<0.05) and higher transfusion rates (RR=2.51, p<0.05). However, no significant difference was noted in the drain blood loss, postoperative Hb levels and VTE events between the two groups. The intravenous and topical routes had comparable efficacy and safety profiles.
The combination of intravenous and topical TXA was relatively more effective in controlling bleeding without increased risk of VTE.
本研究旨在比较静脉、局部和联合使用氨甲环酸(TXA)给药途径对全膝关节置换术(TKA)和全髋关节置换术(THA)患者的失血和输血需求的影响。
这是一项随机对照试验(RCT)的荟萃分析,其中使用加权均数差(WMD)和相对风险(RR)进行数据综合,应用于随机效应模型。还根据手术类型、区域、静脉和局部 TXA 剂量以及输血方案进行了分层分析。主要结局包括术中及总失血量、输血率、术后低血红蛋白(Hb)水平和术后 Hb 下降。然而,次要结局包括住院时间(LOS)和/或静脉血栓栓塞(VTE)的发生。
我们在 PubMed、Embase 和 Cochrane CENTRAL 数据库中检索了比较不同 TXA 给药途径的 RCTs。
接受 TKA 或 THA 的患者。
静脉、局部或联合静脉和局部 TXA。
选择了 26 项 RCT,静脉途径与局部途径在总失血量(WMD=30.92,p=0.31)、引流失血量(WMD=-34.53,p=0.50)、术后 Hb 水平(WMD=-0.01,p=0.96)、Hb 下降(WMD=-0.39,p=0.08)、LOS(WMD=0.15,p=0.38)、输血率(RR=1.08,p=0.75)和 VTE 发生率(RR=1.89,p=0.15)方面无显著差异。与联合给药组相比,单一途径组的总失血量显著增加(WMD=198.07,p<0.05),Hb 下降更大(WMD=0.56,p<0.05),输血率更高(RR=2.51,p<0.05)。然而,两组之间引流失血量、术后 Hb 水平和 VTE 事件无显著差异。静脉和局部途径具有相似的疗效和安全性。
静脉和局部联合使用 TXA 可更有效地控制出血,且不会增加 VTE 的风险。