Schmitt Felix Carl Fabian, Manolov Vasil, Morgenstern Jakob, Fleming Thomas, Heitmeier Stefan, Uhle Florian, Al-Saeedi Mohammed, Hackert Thilo, Bruckner Thomas, Schöchl Herbert, Weigand Markus Alexander, Hofer Stefan, Brenner Thorsten
Department of Anesthesiology, Heidelberg University Hospital, 110, Im Neuenheimer Feld, 69120, Heidelberg, Germany.
Department of Internal Medicine I and Clinical Chemistry, Heidelberg University Hospital, Heidelberg, Germany.
Ann Intensive Care. 2019 Jan 30;9(1):19. doi: 10.1186/s13613-019-0499-6.
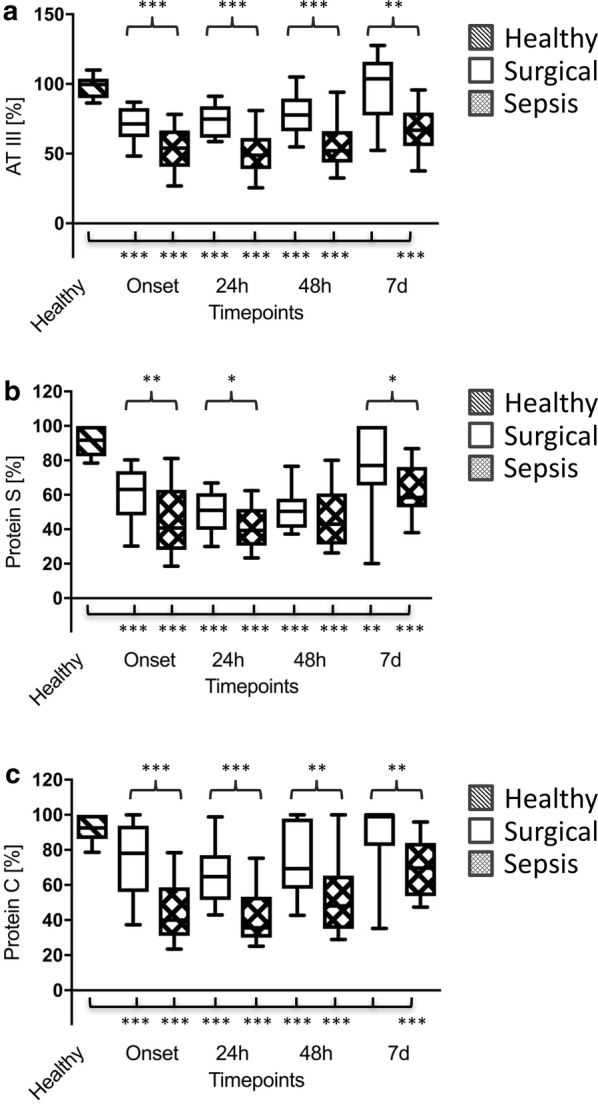
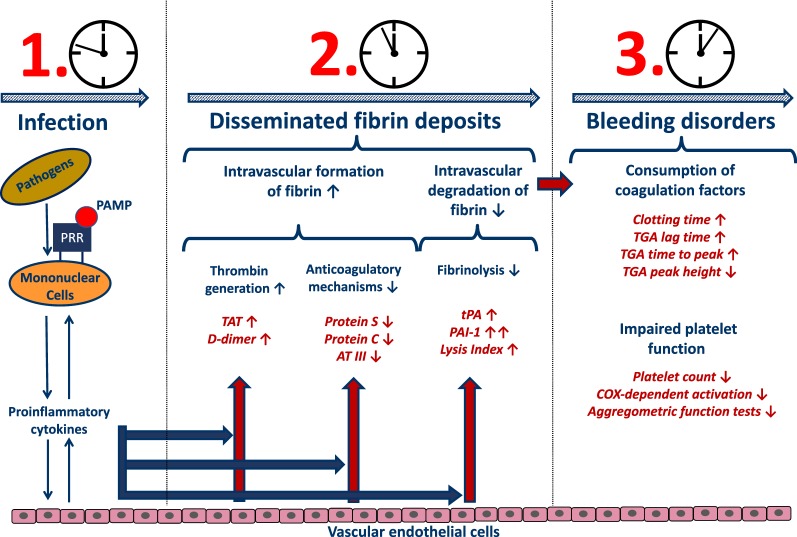
Septic coagulopathy represents a very dynamic disease entity, tilting from initial hypercoagulability towards a subsequent hypocoagulable disease state, entitled overt disseminated intravascular coagulation. Acute fibrinolysis shutdown has recently been described to be a crucial component of initial hypercoagulability in critically ill patients, although the underlying pathomechanisms, the specific temporal kinetics and its outcome relevance in patients with sepsis remain to be determined.
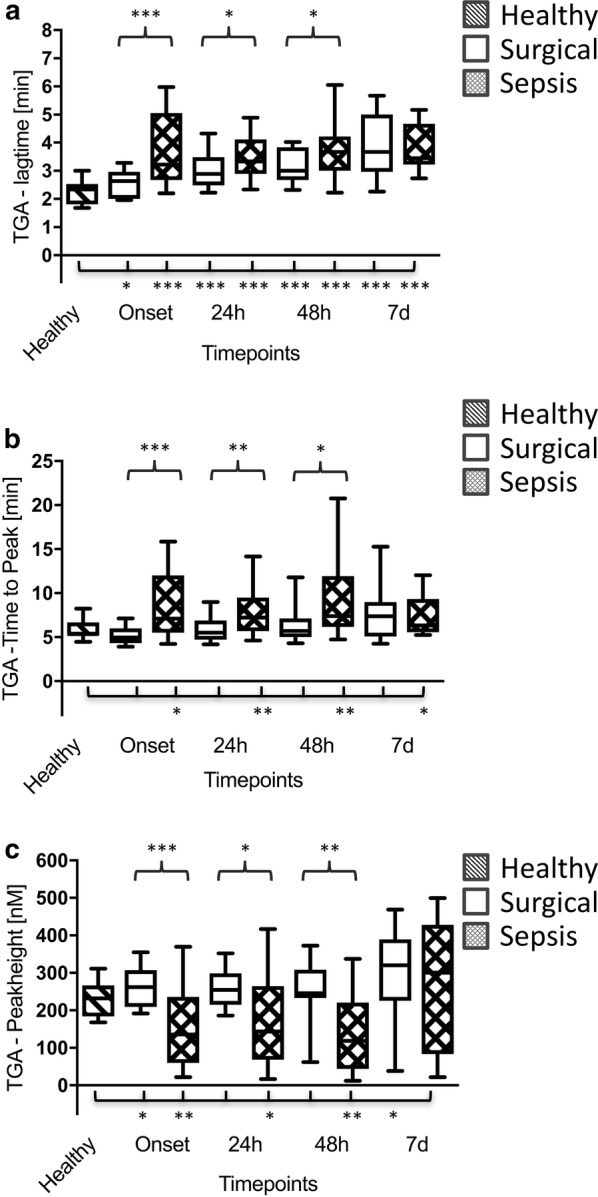
In total, 90 patients (30 with septic shock, 30 surgical controls and 30 healthy volunteers) were enrolled. Blood samples were collected at sepsis onset or prior and immediately after the surgical procedure as well as 3 h, 6 h, 12 h, 24 h, 48 h and 7 d later, whereas blood samples from healthy volunteers were collected once. Besides viscoelastic and aggregometric point-of-care testing (POCT), enzyme-linked immunosorbent and thrombin generation assays and liquid chromatography-mass spectrometry-based measurements were performed.
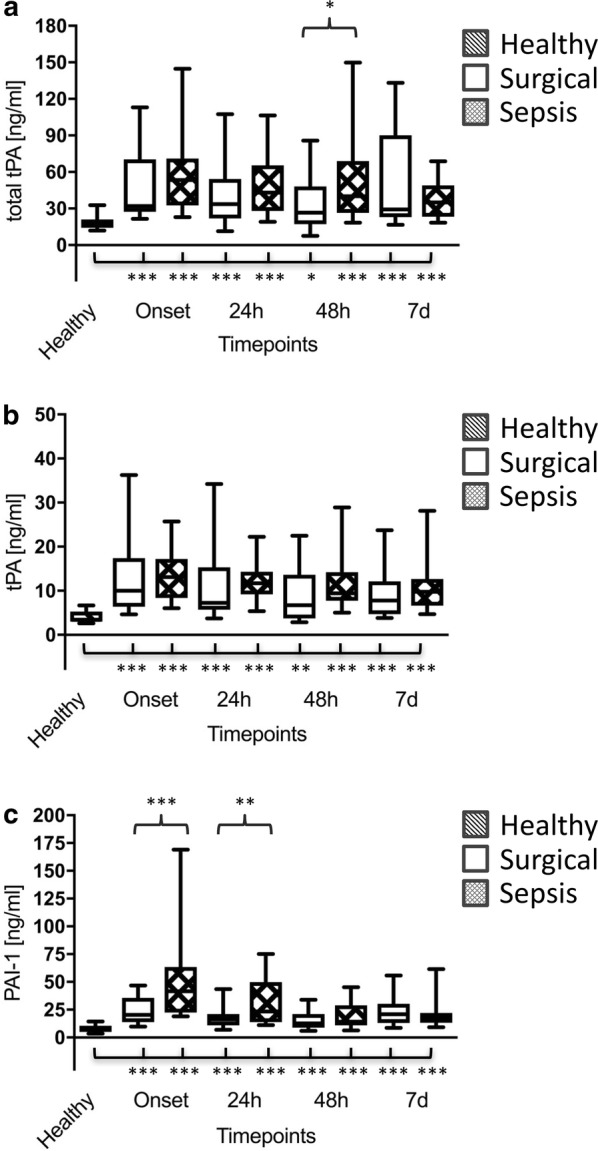
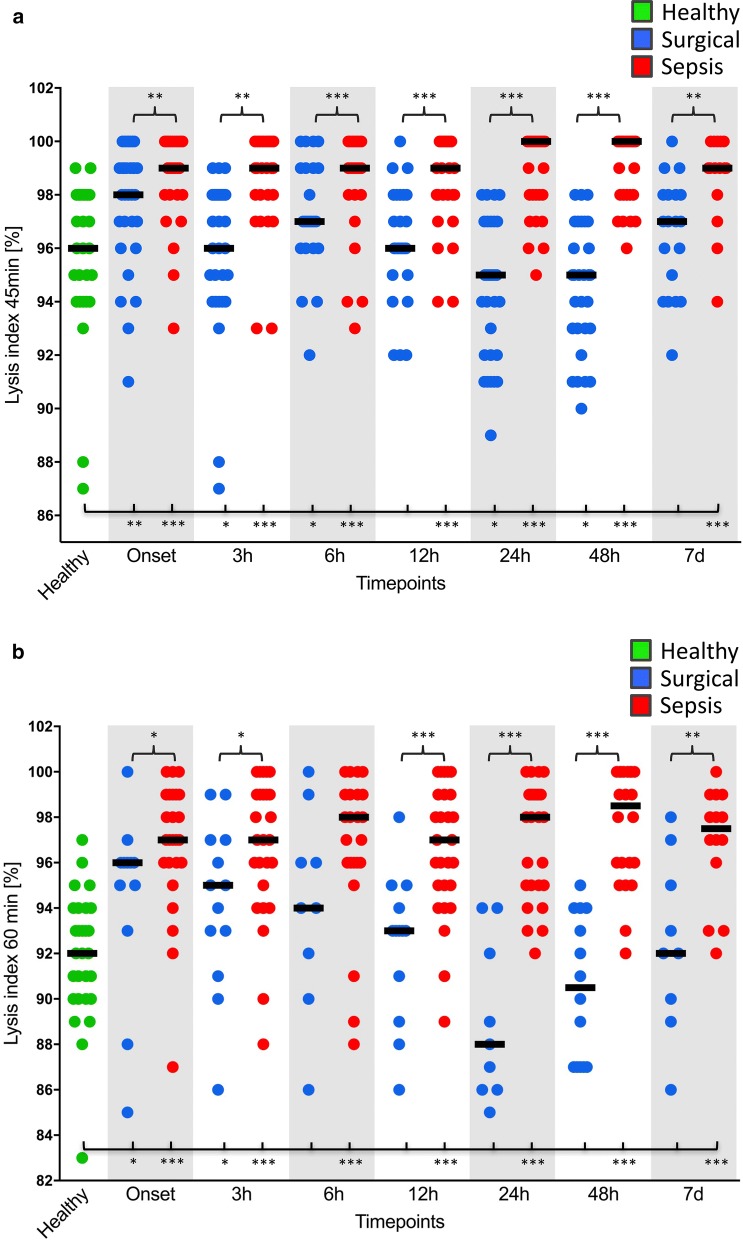
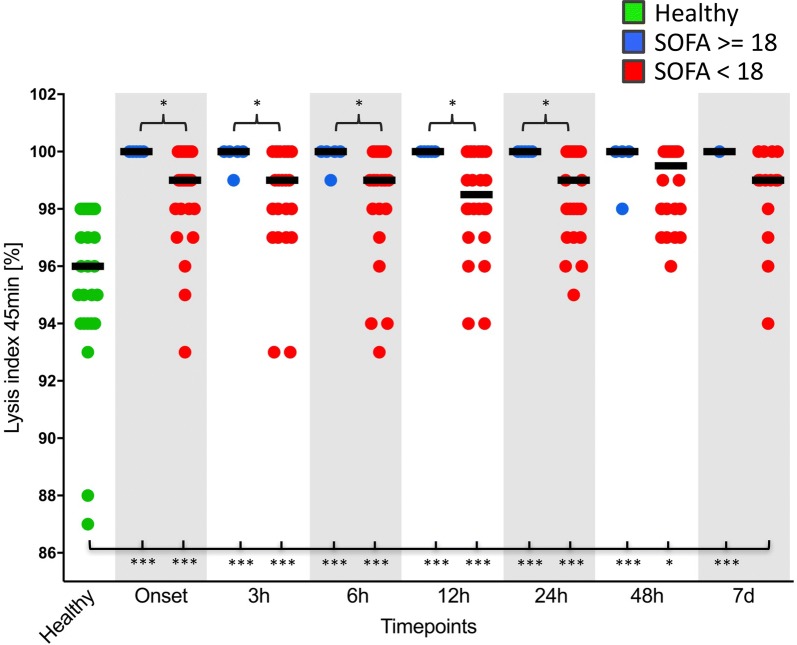
As assessed by viscoelastic POCT, fibrinolysis shutdown occurred early in sepsis. Significant increases in tissue plasminogen activator had no effect on thromboelastometrical lysis indices (LIs). Contrariwise, plasminogen activator inhibitor-1 was already significantly increased at sepsis onset, which was paralleled by significantly increased LIs in patients suffering from septic shock in comparison with both control groups. This effect persisted throughout the 7-day observation period and was most pronounced in severely ill as well as non-surviving septic patients. Thromboelastometrical LI, therefore, proved to be suitable for early diagnosis [e.g. LI 45 min: area under the curve (AUC) up to 0.933] as well as prognosis (e.g. LI 60 min: AUC up to 1.000) of septic shock.
Early inhibition of plasminogen activation leads to acute fibrinolysis shutdown with improved clot stability and is associated with increased morbidity and mortality in septic patients. Trial registration This study was approved by the local ethics committee (Ethics Committee of the Medical Faculty of Heidelberg; Trial-Code No. S247-2014/German Clinical Trials Register (DRKS)-ID: DRKS00008090; retrospectively registered: 07.05.2015). All study patients or their legal representatives signed written informed consent.
脓毒症凝血病是一种非常动态的疾病实体,从最初的高凝状态转变为随后的低凝疾病状态,即显性弥散性血管内凝血。急性纤维蛋白溶解停止最近被描述为危重症患者初始高凝状态的一个关键组成部分,尽管其潜在的发病机制、特定的时间动力学及其在脓毒症患者中的预后相关性仍有待确定。
共纳入90例患者(30例脓毒症休克患者、30例手术对照组患者和30例健康志愿者)。在脓毒症发作时或之前、手术刚结束时以及之后3小时、6小时、12小时、24小时、48小时和7天时采集血样,而健康志愿者的血样仅采集一次。除了进行粘弹性和凝集性即时检验(POCT)外,还进行了酶联免疫吸附试验、凝血酶生成试验以及基于液相色谱 - 质谱的测量。
通过粘弹性POCT评估,纤维蛋白溶解停止在脓毒症早期发生。组织纤溶酶原激活物的显著增加对血栓弹力图溶解指数(LIs)没有影响。相反,纤溶酶原激活物抑制剂 -1在脓毒症发作时就已显著增加,与两个对照组相比,脓毒症休克患者的LIs也显著增加。这种效应在整个7天观察期内持续存在,在重症以及未存活的脓毒症患者中最为明显。因此,血栓弹力图LI被证明适用于脓毒症休克的早期诊断[例如45分钟时的LI:曲线下面积(AUC)高达0.933]以及预后评估(例如60分钟时的LI:AUC高达1.000)。
纤溶酶原激活的早期抑制导致急性纤维蛋白溶解停止,凝块稳定性提高,并与脓毒症患者发病率和死亡率增加相关。试验注册 本研究已获得当地伦理委员会批准(海德堡医学院伦理委员会;试验代码编号:S247 - 2014/德国临床试验注册中心(DRKS)识别号:DRKS00008090;追溯注册日期:2015年5月7日)。所有研究患者或其法定代表人签署了书面知情同意书。