Hoy Wendy E, Reid Christopher M, Huq Molla, McLeod Beverly J, Mott Susan A
Centre for Chronic Disease and NHMRC CKD Centre for Research Excellence, School of Clinical Medicine, Royal Brisbane Clinical School, Faculty of Medicine, The University of Queensland, Brisbane, Queensland, Australia.
School of Public Health, Curtin University, Perth, Western Australia, Australia.
Contemp Clin Trials Commun. 2019 Jan 14;14:100323. doi: 10.1016/j.conctc.2019.100323. eCollection 2019 Jun.
We conducted a double-blind randomised controlled trial in a remote-living Australian Aboriginal group at high risk for chronic disease to assess whether pharmacological treatment with angiotensin converting enzyme inhibitor (ACEi) could delay the onset of albuminuria, hypertension or diabetes in people currently free of those conditions.
Eligibility criteria in 2008 were age ≥18yr, blood pressure ≤140/90 mm/Hg, urinary albumin creatinine ratio (ACR) < 3.4 mg/mmol, normal levels of glycosylated haemoglobin, and, in females, infertility. A 2011 amendment allowed enrolment of fertile females using long-term contraception. "Treatment" was the ACEi perindopril arginine, or placebo, and participant events were ACR ≥3.4 mg/mmol and/or blood pressure >140/90 mm Hg and/or haemoglobin A1c >6.5%, and/or cardiovascular events. Results were analysed in 125 randomised participants who commenced treatment.
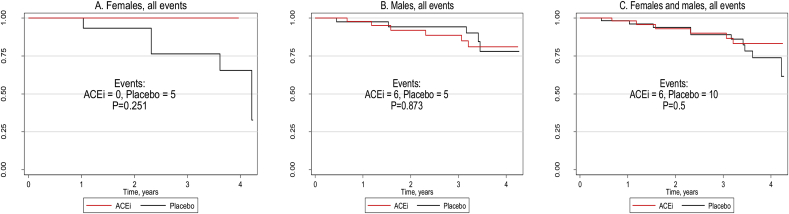
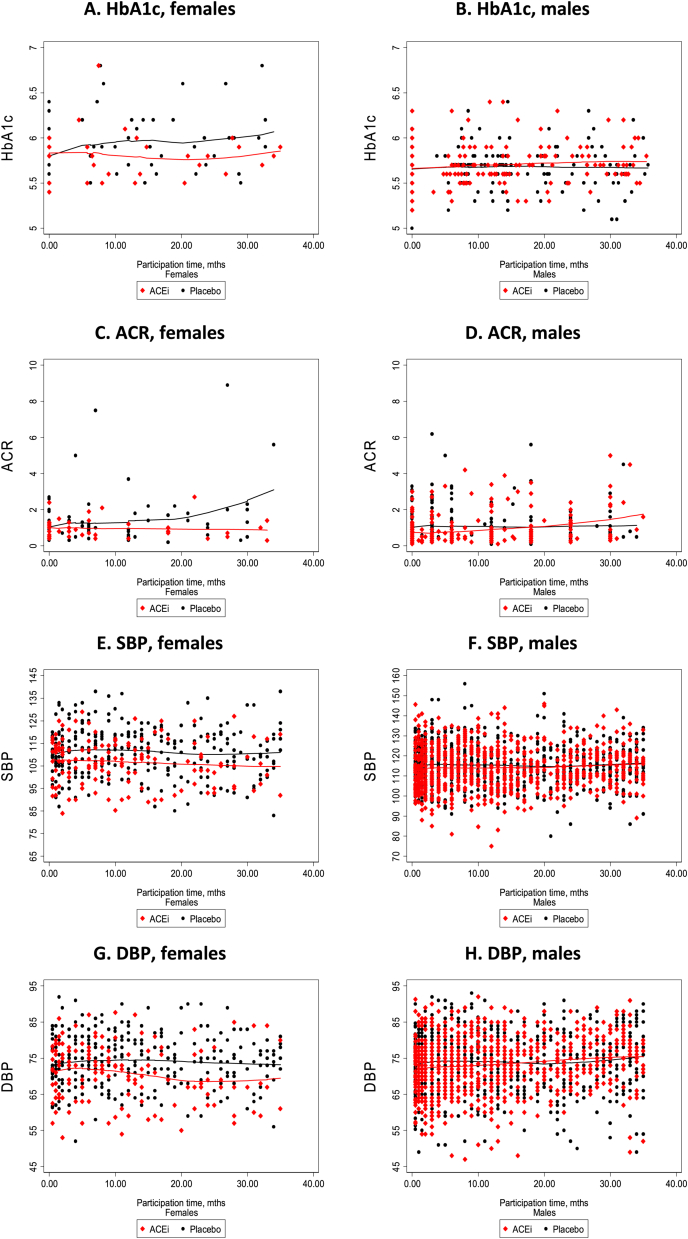
Recruitment was low, especially of women, and dropout rates high: there were finally 60 and 65 people in the ACEi and placebo groups respectively. In females, there were no events among 10 in the ACEi group, versus 5 events among 17 in the placebo group, and longitudinal ACR, HbA1c and blood pressure levels supported probable benefit of ACEi. There was no benefit of ACEi in males, but a probable benefit on diabetes/hypertension events. With the genders combined, there was probable reduction of diabetes (zero vs 4 events, p = 0.068), and of diabetes or hypertension (zero vs 5 events, p = 0.037).
In this high-risk population, ACEi probably delays development of albuminuria, diabetes and hypertension in females, and of non-ACR events overall. Repeat investigation with a larger sample size is warranted.
我们在一个患慢性病风险高的澳大利亚偏远原住民群体中开展了一项双盲随机对照试验,以评估使用血管紧张素转换酶抑制剂(ACEi)进行药物治疗是否可以延缓目前未患蛋白尿、高血压或糖尿病的人群出现这些病症。
2008年的入选标准为年龄≥18岁、血压≤140/90 mmHg、尿白蛋白肌酐比值(ACR)<3.4 mg/mmol、糖化血红蛋白水平正常,女性为不孕。2011年的一项修正案允许纳入使用长效避孕措施的可育女性。“治疗”药物为培哚普利精氨酸(ACEi)或安慰剂,参与者出现的情况为ACR≥3.4 mg/mmol和/或血压>140/90 mmHg和/或糖化血红蛋白A1c>6.5%,和/或心血管事件。对开始治疗的125名随机分组参与者的结果进行了分析。
招募人数较少,尤其是女性,且退出率较高:最终ACEi组和安慰剂组分别有60人和65人。在女性中,ACEi组的10名参与者未出现任何情况,而安慰剂组的17名参与者中有5例出现情况,纵向ACR、糖化血红蛋白和血压水平表明ACEi可能有益。ACEi对男性没有益处,但对糖尿病/高血压事件可能有益。综合两性情况,糖尿病可能减少(0例对4例,p = 0.068),糖尿病或高血压可能减少(0例对5例,p = 0.037)。
在这个高风险人群中,ACEi可能会延缓女性蛋白尿、糖尿病和高血压的发展,以及总体非ACR事件的发展。有必要用更大的样本量进行重复研究。