Garg Mayur, Royce Simon G, Tikellis Chris, Shallue Claire, Sluka Pavel, Wardan Hady, Hosking Patrick, Monagle Shaun, Thomas Merlin, Lubel John S, Gibson Peter R
Department of Gastroenterology, Eastern Health Clinical School, Monash University, Level 3W, Building B, 8 Arnold St, Box Hill, Victoria, 3128, Australia.
Department of Medicine, Central Clinical School, Monash University, Victoria, Australia.
Therap Adv Gastroenterol. 2019 Jan 18;12:1756284818822566. doi: 10.1177/1756284818822566. eCollection 2019.
The intestinal vitamin D receptor (VDR) remains poorly characterized in patients with inflammatory bowel disease (IBD).
Colonoscopic biopsies and intestinal resection specimens from the terminal ileum, ascending and sigmoid colon, from patients with and without IBD, were analyzed for VDR mRNA quantification by polymerase chain reaction, and protein localization and semi-quantification by immunohistochemistry. The relationship between VDR and intestinal inflammation, serum 25(OH)D and oral vitamin D intake was elicited.
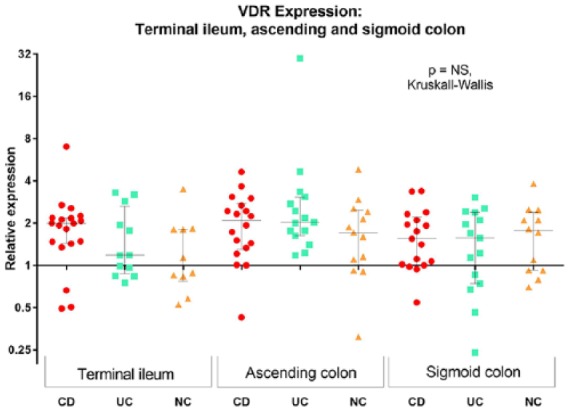
A total of 725 biopsies from 20 patients with Crohn's disease (CD), 15 with ulcerative colitis (UC) and 14 non-IBD controls who underwent colonoscopy were studied. VDR gene expression and protein staining intensity was similar across all three groups, and across the intestinal segments. Sigmoid colon VDR mRNA expression inversely correlated with faecal calprotectin ( = -0.64, = 0.026) and histological score ( = -0.67, = 0.006) in UC, and histological score ( = -0.58, = 0.019) in patients with CD. VDR staining intensity was higher in quiescent than diseased segments. No relationship with serum 25(OH)D or oral vitamin D intake was noted. Immunohistochemical staining of 28 intestinal resection specimens from 15 patients (5 each with CD, UC and non-IBD controls) showed diffuse VDR staining in the mucosa, submucosa and circular muscle.
VDR transcript expression and protein staining intensity are inversely related to inflammation in IBD, but unrelated to serum 25(OH)D, and similar to non-IBD controls. Strategies to upregulate intestinal VDR, potentially translating to modulation of disease activity, require investigation.
炎症性肠病(IBD)患者肠道维生素D受体(VDR)的特征仍不清楚。
通过聚合酶链反应分析来自有或无IBD患者的结肠镜活检组织以及回肠末端、升结肠和乙状结肠的肠切除标本中的VDR mRNA定量,并通过免疫组织化学分析蛋白质定位和半定量。探讨VDR与肠道炎症、血清25(OH)D和口服维生素D摄入量之间的关系。
共研究了20例克罗恩病(CD)患者、15例溃疡性结肠炎(UC)患者和14例接受结肠镜检查的非IBD对照者的725份活检组织。三组以及各肠段的VDR基因表达和蛋白染色强度相似。在UC中,乙状结肠VDR mRNA表达与粪便钙卫蛋白呈负相关(r = -0.64,P = 0.026),与组织学评分呈负相关(r = -0.67,P = 0.006);在CD患者中,与组织学评分呈负相关(r = -0.58,P = 0.019)。静止期肠段的VDR染色强度高于病变肠段。未发现与血清25(OH)D或口服维生素D摄入量有关。对15例患者(CD、UC和非IBD对照各5例)的28份肠切除标本进行免疫组织化学染色,结果显示黏膜、黏膜下层和环形肌层均有弥漫性VDR染色。
VDR转录本表达和蛋白染色强度与IBD中的炎症呈负相关,但与血清25(OH)D无关,且与非IBD对照相似。上调肠道VDR的策略可能转化为对疾病活动的调节,需要进一步研究。