Yang Lu-Ping, Wang Zi-Xian, He Ming-Ming, Jin Ying, Ren Chao, Wang Zhi-Qiang, Wang Feng-Hua, Li Yu-Hong, Wang Feng, Xu Rui-Hua
Department of Medical Oncology, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, China.
J Cancer. 2019 Jan 1;10(3):602-610. doi: 10.7150/jca.28842. eCollection 2019.
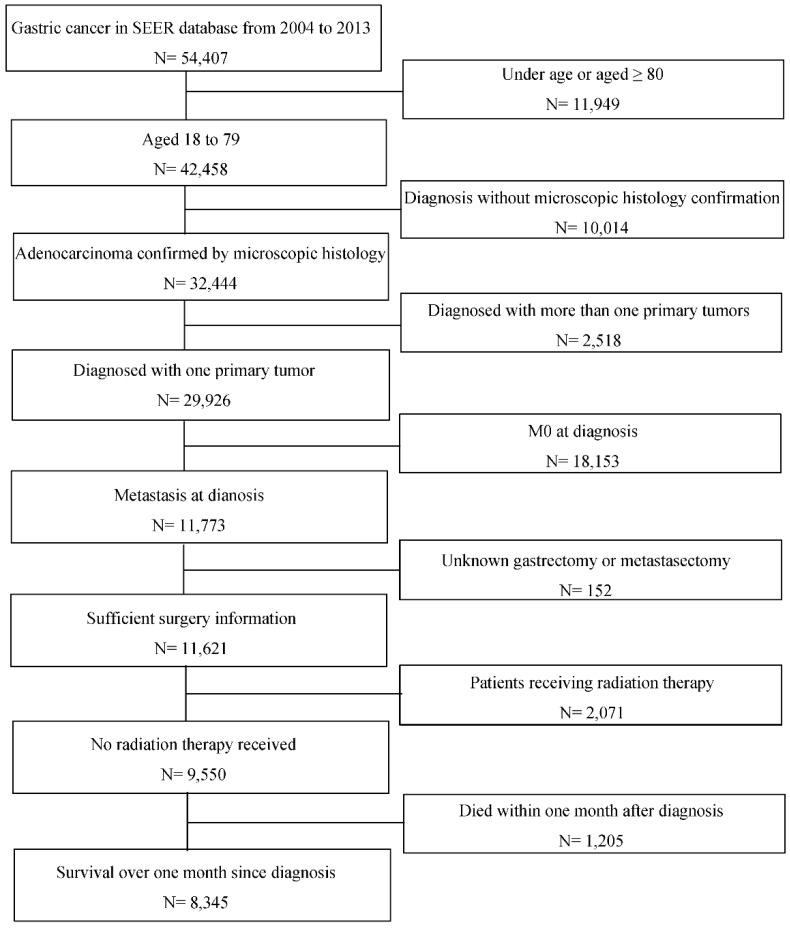
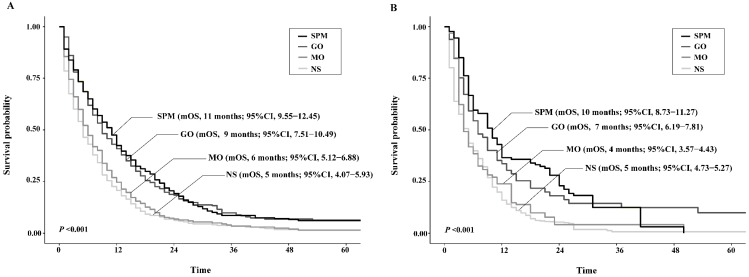
Palliative surgeries were controversial for asymptomatic metastatic gastric cancer (mGC) patients. This study was aimed to evaluate survival benefit of palliative surgeries to gastric and/or metastatic tumors in mGC patients based on U.S population. A total of 8345 gastric cancer patients diagnosed with synchronous distal metastasis between 2004 to 2013 from the Surveillance, Epidemiology, and End Results Program (SEER) database were divided into four groups according to surgery strategies: surgeries to both primary and metastatic tumors (SPM), gastrectomy only (GO), metastasectomy only (MO) and no surgery performed (NS). Their clinicopathological characteristics and overall survival (OS) were analyzed before and after propensity score matching (PSM) and coarsened exact matching (CEM). The median OS of SPM and GO patients was both significantly higher than NS patients (11 months vs. 8 months vs. 5 months; <0.001, respectively) while that of MO was not (6 months vs. 5 months; = 0.286). In comparisons between surgery strategies, survival benefit was similar between SPM and GO groups (=0.389) and both showed significantly better survival than MO patients (<0.001). All surgery strategies were proved to be favorable prognostic factors over non-surgical treatment (Hazard ratio (HR) for SPM: 0.60, <0.001; HR for GO: 0.62, <0.001; HR for MO: 0.91, =0.046). Similar results were obtained after matching by PSM and CEM except that prognostic impact of MO deteriorated. Gastrectomy plus metastasectomy or gastrectomy alone could be adopted as a choice of improving survival in the U.S population. Metastasectomy alone is not generally recommended.
姑息性手术对于无症状的转移性胃癌(mGC)患者存在争议。本研究旨在基于美国人群评估姑息性手术对mGC患者的胃部和/或转移性肿瘤的生存获益。从监测、流行病学和最终结果计划(SEER)数据库中选取了2004年至2013年期间诊断为同步远端转移的8345例胃癌患者,根据手术策略分为四组:原发肿瘤和转移瘤均手术(SPM)、仅行胃切除术(GO)、仅行转移瘤切除术(MO)和未进行手术(NS)。在倾向得分匹配(PSM)和粗化精确匹配(CEM)前后分析了他们的临床病理特征和总生存期(OS)。SPM组和GO组患者的中位OS均显著高于NS组患者(分别为11个月 vs. 8个月 vs. 5个月;P均<0.001),而MO组则不然(6个月 vs. 5个月;P = 0.286)。在手术策略之间的比较中,SPM组和GO组的生存获益相似(P = 0.389),且两者的生存期均显著优于MO组患者(P<0.001)。所有手术策略均被证明是优于非手术治疗的有利预后因素(SPM的风险比(HR):0.60,P<0.001;GO的HR:0.62,P<0.001;MO的HR:0.91,P = 0.046)。通过PSM和CEM匹配后得到了类似的结果,只是MO的预后影响有所恶化。胃切除术加转移瘤切除术或单纯胃切除术可作为改善美国人群生存率的一种选择。一般不推荐仅行转移瘤切除术。