Centre for Cancer Prevention, Wolfson Institute of Preventive Medicine, Barts & The London School of Medicine and Dentistry, Queen Mary University of London, London, UK
School of Cancer and Pharmaceutical Sciences, Faculty of Life Sciences and Medicine, King's College London, London SE1 9RT, UK.
BMJ. 2019 Feb 6;364:l240. doi: 10.1136/bmj.l240.
To provide the first report on the main outcomes from the prevalence and incidence rounds of a large pilot of routine primary high risk human papillomavirus (hrHPV) testing in England, compared with contemporaneous primary liquid based cytology screening.
Observational study.
The English Cervical Screening Programme.
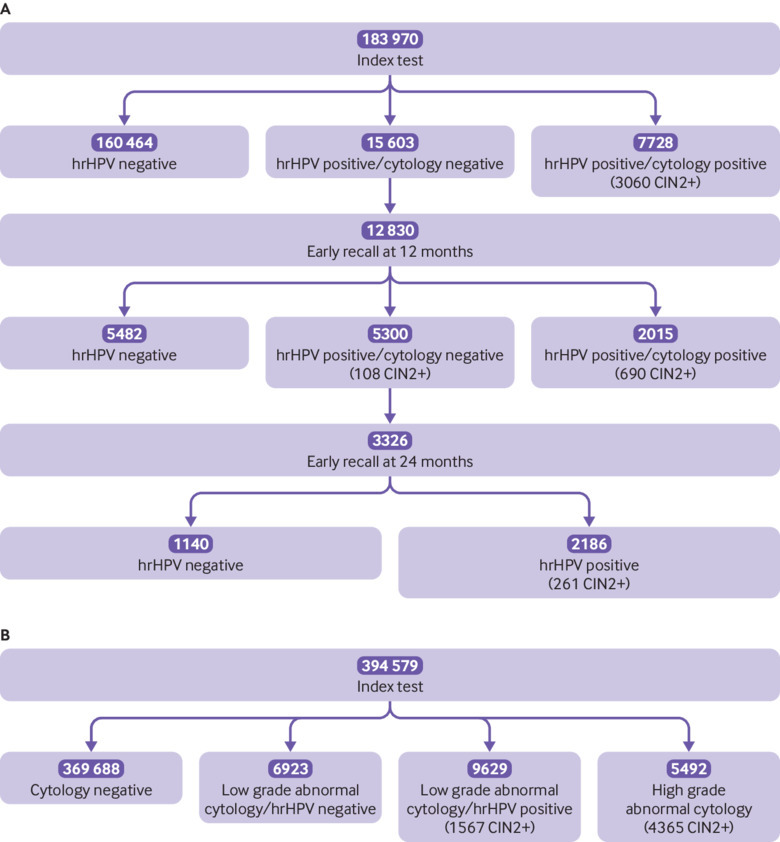
578 547 women undergoing cervical screening in primary care between May 2013 and December 2014, with follow-up until May 2017; 183 970 (32%) were screened with hrHPV testing.
Routine cervical screening with hrHPV testing with liquid based cytology triage and two early recalls for women who were hrHPV positive and cytology negative, following the national screening age and interval recommendations.
Frequency of referral for a colposcopy; adherence to early recall; and relative detection of cervical intraepithelial neoplasia grade 2 or worse from hrHPV testing compared with liquid based cytology in two consecutive screening rounds.
Baseline hrHPV testing and early recall required approximately 80% more colposcopies, (adjusted odds ratio 1.77, 95% confidence interval 1.73 to 1.82), but detected substantially more cervical intraepithelial neoplasia than liquid based cytology (1.49 for cervical intraepithelial neoplasia grade 2 or worse, 1.43 to 1.55; 1.44 for cervical intraepithelial neoplasia grade 3 or worse, 1.36 to 1.51) and for cervical cancer (1.27, 0.99 to 1.63). Attendance at early recall and colposcopy referral were 80% and 95%, respectively. At the incidence screen, the 33 506 women screened with hrHPV testing had substantially less cervical intraepithelial neoplasia grade 3 or worse than the 77 017 women screened with liquid based cytology (0.14, 0.09 to 0.23).
In England, routine primary hrHPV screening increased the detection of cervical intraepithelial neoplasia grade 3 or worse and cervical cancer by approximately 40% and 30%, respectively, compared with liquid based cytology. The very low incidence of cervical intraepithelial neoplasia grade 3 or worse after three years supports extending the screening interval.
报告英格兰大规模常规高危型人乳头瘤病毒(hrHPV)检测初步流行率和发病率研究的主要结果,该研究与同期的液基细胞学初级筛查进行了比较。
观察性研究。
英国宫颈筛查计划。
2013 年 5 月至 2014 年 12 月期间在初级保健中接受宫颈筛查的 578547 名女性,随访至 2017 年 5 月;其中 183970 名(32%)接受了 hrHPV 检测。
按照国家筛查年龄和间隔建议,对常规宫颈筛查采用液基细胞学联合 hrHPV 检测进行分流,对 hrHPV 阳性和细胞学阴性的女性进行两次早期召回。
阴道镜检查转诊率;早期召回的依从性;以及在连续两轮筛查中,与液基细胞学相比,hrHPV 检测对宫颈上皮内瘤变 2 级或更高级别病变的相对检出率。
基线 hrHPV 检测和早期召回需要增加约 80%的阴道镜检查(调整后的优势比 1.77,95%置信区间 1.73 至 1.82),但与液基细胞学相比,检测到更多的宫颈上皮内瘤变(宫颈上皮内瘤变 2 级或更高级别病变 1.49,1.43 至 1.55;宫颈上皮内瘤变 3 级或更高级别病变 1.44,1.36 至 1.51)和宫颈癌(1.27,0.99 至 1.63)。早期召回和阴道镜检查转诊的依从率分别为 80%和 95%。在发病筛查中,与液基细胞学筛查的 77017 名女性相比,接受 hrHPV 检测的 33506 名女性的宫颈上皮内瘤变 3 级或更高级别病变明显减少(0.14,0.09 至 0.23)。
在英格兰,与液基细胞学相比,常规初级 hrHPV 筛查使宫颈上皮内瘤变 3 级或更高级别病变和宫颈癌的检出率分别增加了约 40%和 30%。三年后宫颈上皮内瘤变 3 级或更高级别病变的发病率非常低,支持延长筛查间隔。