Zhang Xuancheng, Xie Guoming, Zhang Chengyuan, Fang Zhaoyi, Zhao Jinzhong, Huangfu Xiaoqiao
Department of Sports Medicine, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, 600 Yishan Road, Shanghai, 200233, China.
BMC Musculoskelet Disord. 2019 Feb 7;20(1):53. doi: 10.1186/s12891-019-2439-x.
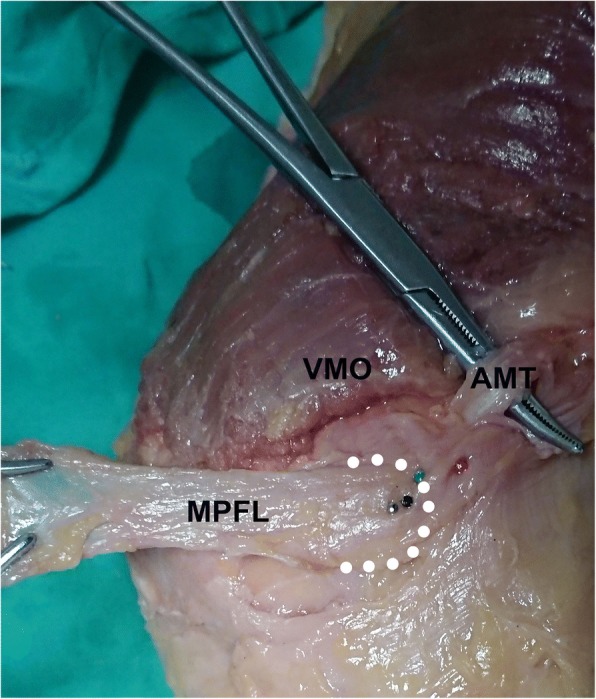
In anatomic medial patellofemoral ligament (MPFL) reconstruction, malpositioning of the MPFL femoral tunnel is common. A palpable sulcus reportedly exists at the anatomic femoral attachment of the MPFL. The present study aimed to investigate the accuracy of the sulcus localization method to establish the MPFL femoral tunnel.
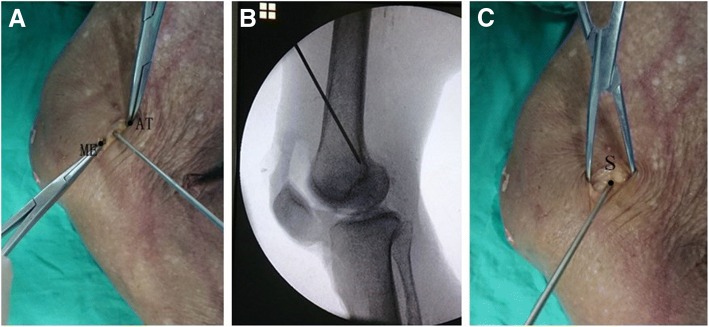
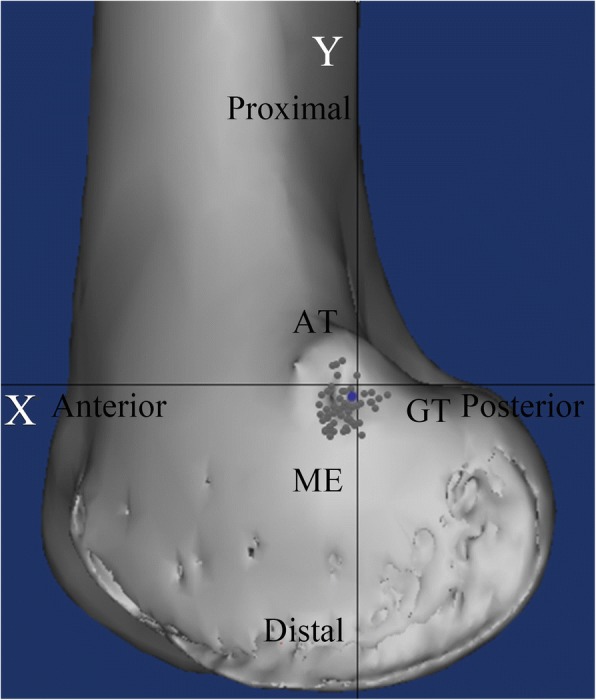
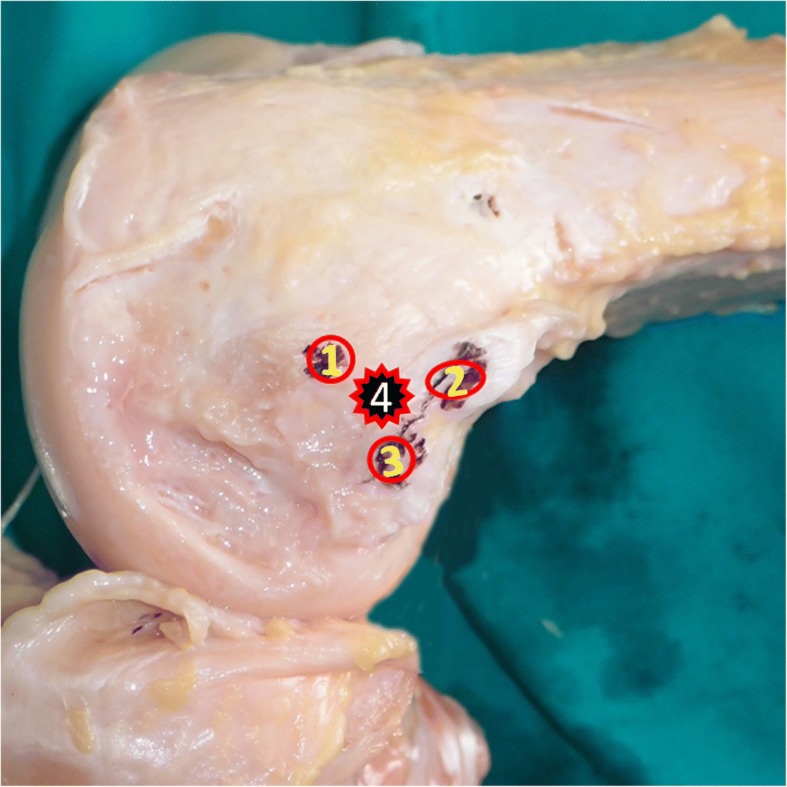
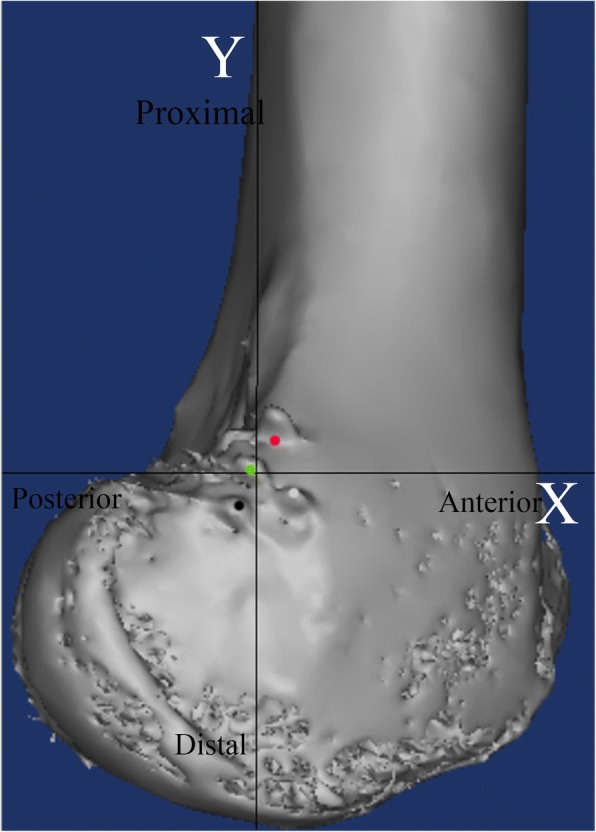
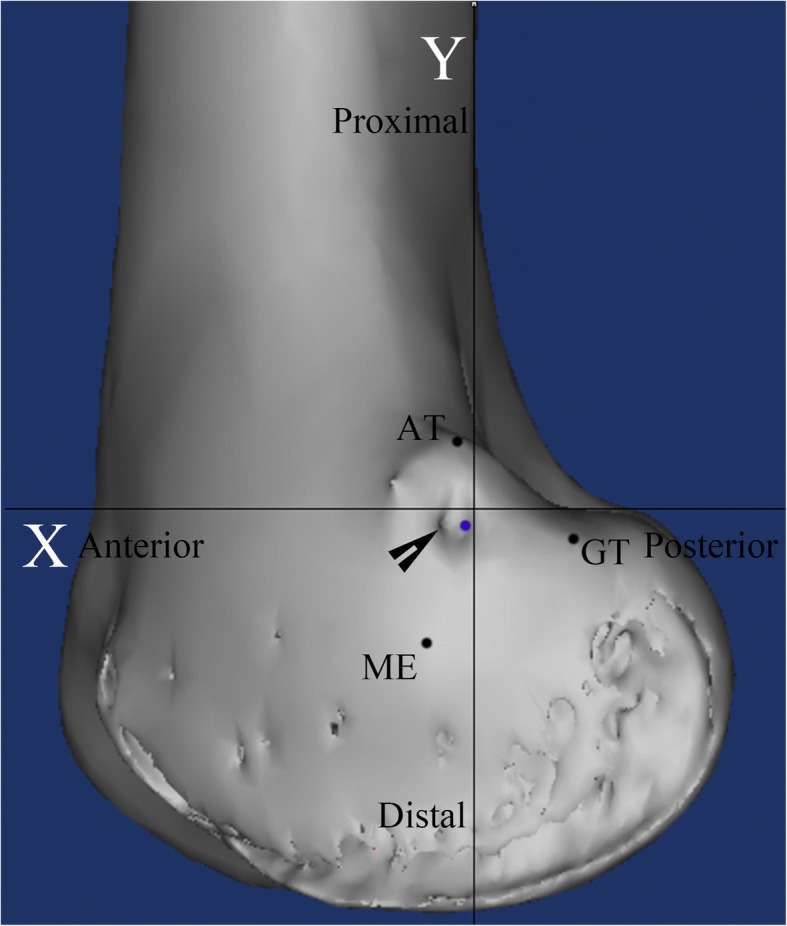
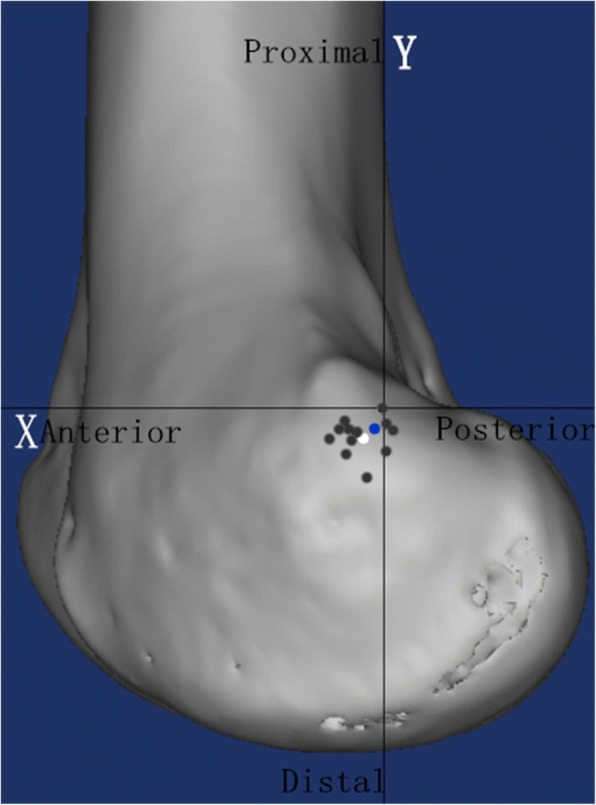
A cadaveric study was first done on 12 knees to evaluate the accuracy of the sulcus localization method to establish the entry points of the MPFL femoral tunnel in comparison with the midpoint and fluoroscopic localization methods. The center of the native MPFL femoral attachment was served as the reference in the cadaveric study. A clinical study was then performed to further evaluate the accuracy of the sulcus localization method in 53 patients (60 knees). Schöttle's point was served as the reference in the clinical study. Femoral tunnel placement was defined as accurate when it was less than 5 mm from Schöttle's point. In both the cadaveric and clinical studies, MPFL femoral tunnel placement was assessed on postoperative reconstructed three-dimensional computed tomography images. In the cadaveric study, the accuracy of different localization methods was compared using analysis of variance.
In the cadaveric study, the mean distances from the native MPFL attachment to the femoral tunnel entry point were 4.2 ± 1.0 mm (range 2.4-5.6 mm), 4.4 ± 1.4 mm (range 1.8-6.6 mm) and 2.9 ± 0.8 mm (range 1.9-4.4 mm) using the midpoint, fluoroscopic, and sulcus localization methods, respectively; this distance significantly differed between the midpoint and sulcus localization methods, and between the fluoroscopic and sulcus localization methods (p ≤ .05). While there were no significant differences between the midpoint and fluoroscopic localization methods (n.s.). In the clinical study, the mean distance between the femoral tunnel and Schöttle's point was 3.5 ± 1.5 mm (range 0.4-6.1 mm), with accurate tunnel placement achieved in 49 of 60 cases (82%).
The sulcus localization method can accurately guide MPFL femoral tunnel placement. This method might be useful for orthopedic surgeons.
IV.
在解剖学内侧髌股韧带(MPFL)重建术中,MPFL股骨隧道位置不当很常见。据报道,在MPFL的解剖学股骨附着处存在一个可触及的沟。本研究旨在探讨利用沟定位法建立MPFL股骨隧道的准确性。
首先对12具膝关节进行尸体研究,与中点定位法和透视定位法相比,评估沟定位法建立MPFL股骨隧道入口点的准确性。在尸体研究中,以天然MPFL股骨附着点的中心作为参考。然后对53例患者(60个膝关节)进行临床研究,进一步评估沟定位法的准确性。在临床研究中,以朔特勒点作为参考。当股骨隧道位置距离朔特勒点小于5毫米时,定义为放置准确。在尸体研究和临床研究中,均在术后重建的三维计算机断层扫描图像上评估MPFL股骨隧道的位置。在尸体研究中,使用方差分析比较不同定位方法的准确性。
在尸体研究中,使用中点定位法、透视定位法和沟定位法时,从天然MPFL附着点到股骨隧道入口点的平均距离分别为4.2±1.0毫米(范围2.4 - 5.6毫米)、4.4±1.4毫米(范围1.8 - 6.6毫米)和2.9±0.8毫米(范围1.9 - 4.4毫米);中点定位法与沟定位法之间以及透视定位法与沟定位法之间的该距离存在显著差异(p≤0.05)。而中点定位法与透视定位法之间无显著差异(无统计学意义)。在临床研究中,股骨隧道与朔特勒点之间的平均距离为3.5±1.5毫米(范围0.4 - 6.1毫米),60例中有49例(82%)实现了隧道的准确放置。
沟定位法可准确指导MPFL股骨隧道的放置。该方法可能对骨科医生有用。
IV级。