Department of Medicine (Geriatrics), University College Cork, Cork University Hospital, Cork, Ireland.
Health Economics, University of East Anglia Medical School, Norwich, England.
BMC Geriatr. 2019 Feb 13;19(1):40. doi: 10.1186/s12877-019-1047-9.
The aim of this trial is to evaluate the effect of SENATOR software on incident, adverse drug reactions (ADRs) in older, multimorbid, hospitalized patients. The SENATOR software produces a report designed to optimize older patients' current prescriptions by applying the published STOPP and START criteria, highlighting drug-drug and drug-disease interactions and providing non-pharmacological recommendations aimed at reducing the risk of incident delirium.
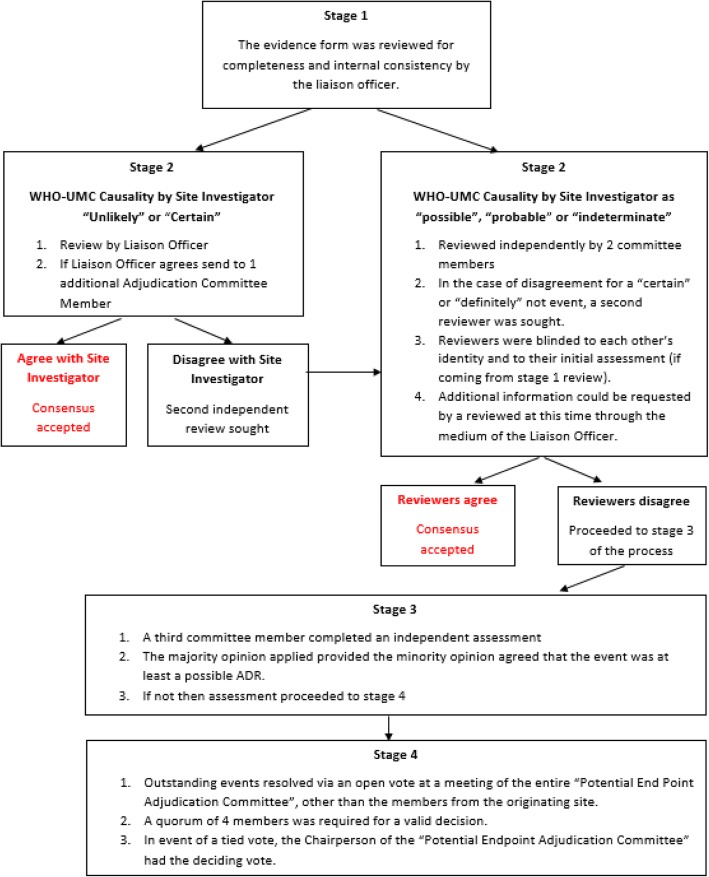
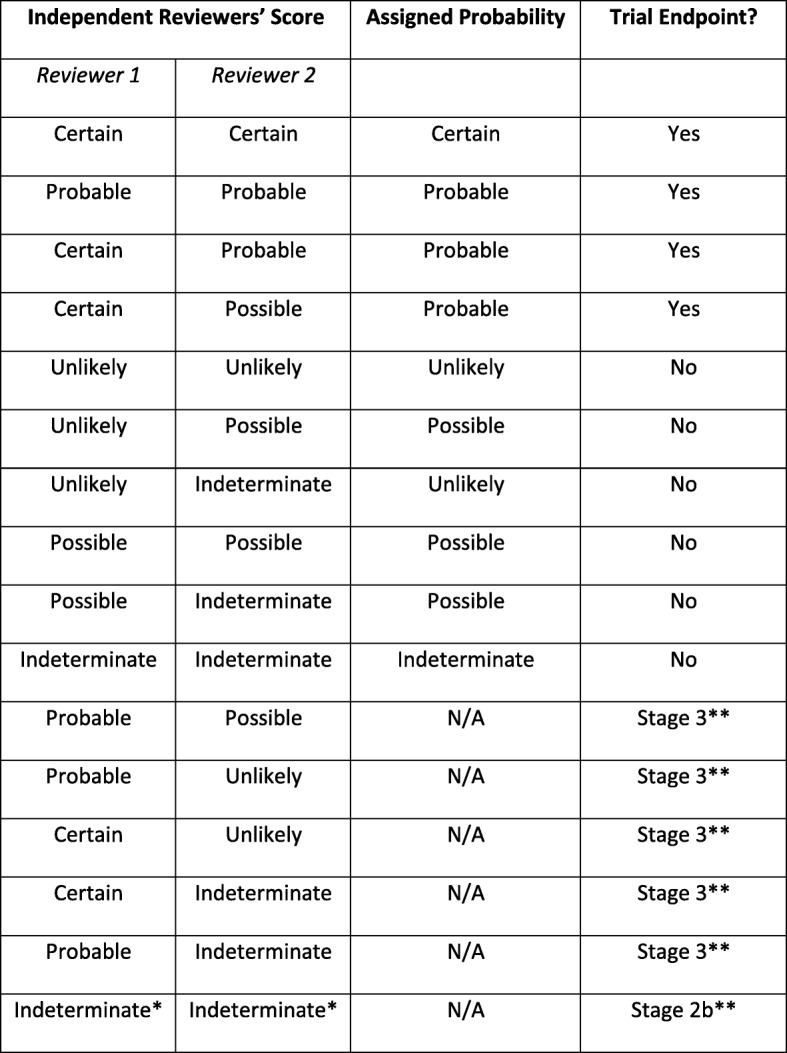
We will conduct a multinational, pragmatic, parallel arm Prospective Randomized Open-label, Blinded Endpoint (PROBE) controlled trial. Patients with acute illnesses are screened for recruitment within 48 h of arrival to hospital and enrolled if they meet the relevant entry criteria. Participants' medical history, current prescriptions, select laboratory tests, electrocardiogram, cognitive status and functional status are collected and entered into a dedicated trial database. Patients are individually randomized with equal allocation ratio. Randomization is stratified by site and medical versus surgical admission, and uses random block sizes. Patients randomized to either arm receive standard routine pharmaceutical clinical care as it exists in each site. Additionally, in the intervention arm an individualized SENATOR-generated medication advice report based on the participant's clinical and medication data is placed in their medical record and a senior medical staff member is requested to review it and adopt any of its recommendations that they judge appropriate. The trial's primary outcome is the proportion of patients experiencing at least one adjudicated probable or certain, non-trivial ADR, during the index hospitalization, assessed at 14 days post-randomization or at index hospital discharge if it occurs earlier. Potential ADRs are identified retrospectively by the site researchers who complete a Potential Endpoint Form (one per type of event) that is adjudicated by a blinded, expert committee. All occurrences of 12 pre-specified events, which represent the majority of ADRs, are reported to the committee along with other suspected ADRs. Participants are followed up 12 (+/- 4) weeks post-index hospital discharge to assess medication quality and healthcare utilization. This is the first clinical trial to examine the effectiveness of a software intervention on incident ADRs and associated healthcare costs during hospitalization in older people with multi-morbidity and polypharmacy.
Clinicaltrials.gov NCT02097654 , 27 March 2014.
本试验旨在评估 SENATOR 软件对老年、多病、住院患者新发不良药物反应(ADR)的影响。SENATOR 软件生成一份报告,旨在通过应用已发表的 STOPP 和 START 标准优化老年患者的现有处方,突出药物-药物和药物-疾病相互作用,并提供非药物建议,以降低新发谵妄的风险。
我们将进行一项多中心、实用、平行臂前瞻性随机开放标签、盲终点(PROBE)对照试验。在患者入院后 48 小时内筛选入组,符合相关入组标准的患者纳入研究。采集患者的病史、当前用药、部分实验室检查、心电图、认知状态和功能状态,并录入专门的试验数据库。患者按个体进行随机分组,分配比例为 1:1。随机分组按地点和内科或外科入院分层,采用随机分组块大小。随机分至两组的患者均接受各入组地点标准常规药物治疗。此外,在干预组中,根据患者的临床和药物数据生成一份个体化的 SENATOR 生成的药物建议报告,放入患者的病历中,并要求一名高级医务人员审查该报告并采用他们认为合适的任何建议。试验的主要结局是在 14 天随机分组后或更早的索引住院出院时,评估索引住院期间至少发生 1 例经判定为可能或确定、非轻微 ADR 的患者比例。潜在 ADR 由地点研究人员通过填写潜在终点表格(每种事件一份)来回顾性识别,该表格由盲法、专家委员会进行判定。委员会会对代表大部分 ADR 的 12 种预先指定事件的所有发生情况以及其他疑似 ADR 进行报告。患者在索引住院出院后 12 周(+/-4 周)进行随访,以评估药物质量和医疗保健利用情况。这是第一项评估软件干预对老年人多病和多药治疗时新发 ADR 及相关医疗费用影响的临床试验。
Clinicaltrials.gov NCT02097654,2014 年 3 月 27 日。