Kim Hyun Jung, Choi Seung Ho, Eum Darhae, Kim Seung Hyun
Institute for Evidence-based Medicine, Department of Preventive Medicine, College of Medicine, Korea University.
Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Severance Hospital.
Medicine (Baltimore). 2019 Feb;98(7):e14339. doi: 10.1097/MD.0000000000014339.
Adequate intravenous fluid replacement is recommended as an effective nonpharmacologic strategy for reducing postoperative nausea and vomiting (PONV), one of the most common and stressful complications of general anesthesia. We aimed to evaluate the effect of hydration, according to the type of fluid, on PONV as previous studies have reported inconsistent results.
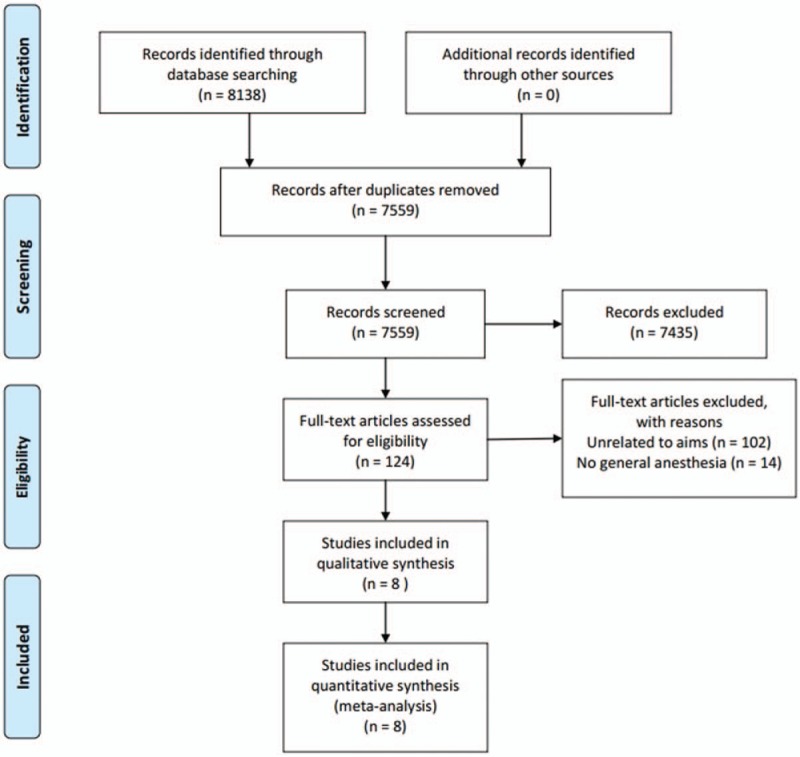
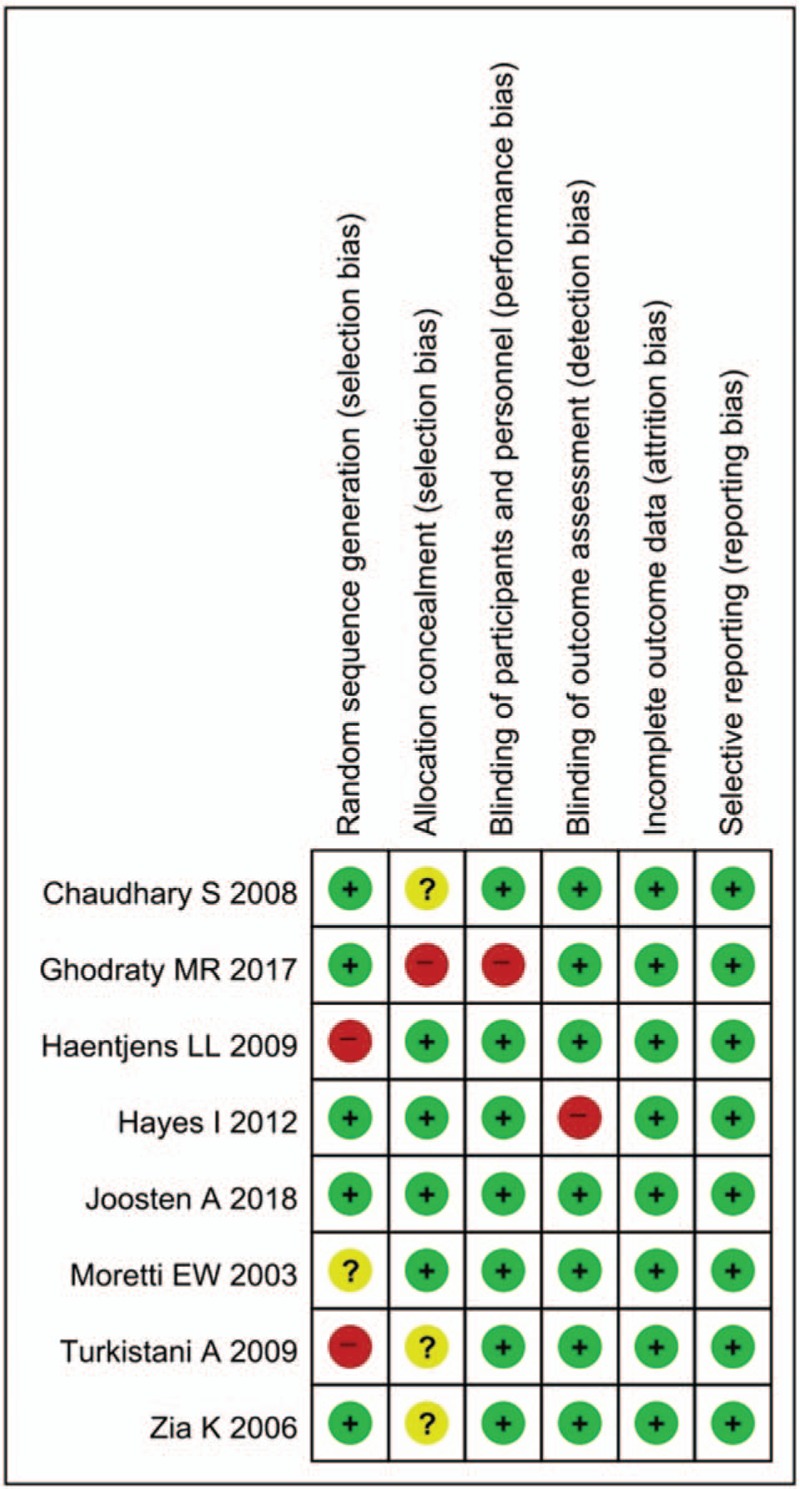
We performed a systemic review and meta-analysis of randomized controlled trials (RCTs) comparing infusion of colloid with that of crystalloid in terms of PONV incidence and the need for rescue antiemetic therapies for 24 hours after surgery under general anesthesia. The effect of fluid infusion according to the duration of anesthesia was also examined. A literature search was performed, using MEDLINE, Excerpta Medica Database, Cochrane Central Register of Controlled Trials, Web of Science, and Scopus, up to February 2018.
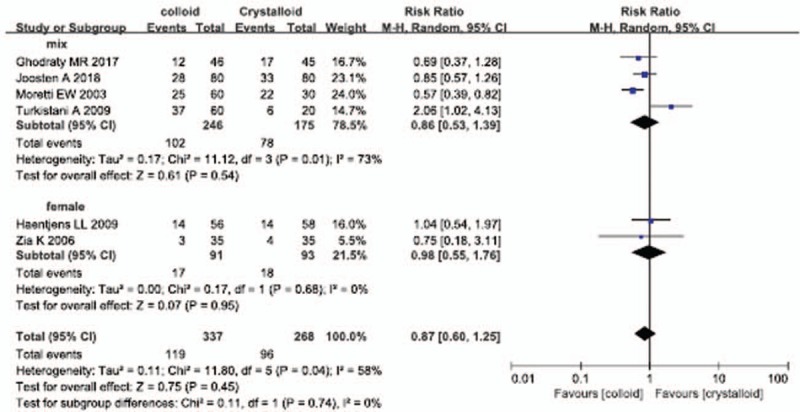
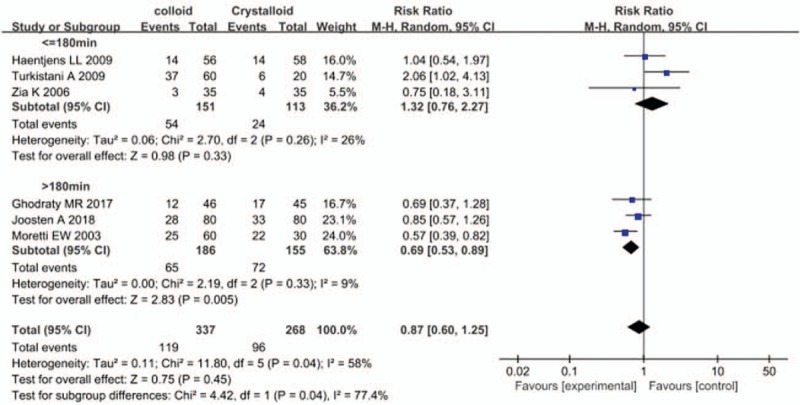
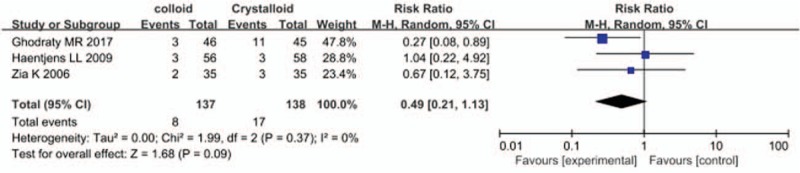
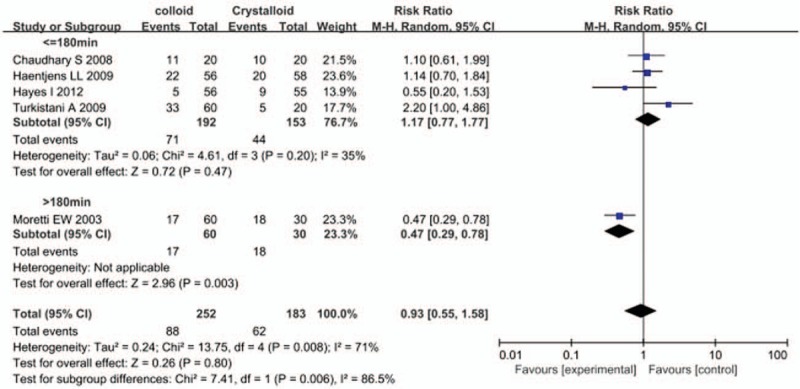
We included 8 RCTs. Compared with the crystalloid infusion, perioperative colloid infusion did not reduce PONV incidence, with a relative risk of 0.87 (95% confidence interval [CI], 0.60-1.25). However, subgroup analysis by duration of anesthesia showed a statistically significant subgroup effect (P = .04, I = 77.4%), suggesting that the effect of colloid differed from that of crystalloid depending on the duration of anesthesia. In the subgroup that underwent anesthesia for more than 3 hours, in which the patients had mostly undergone abdominal surgeries, colloid infusion significantly reduced the incidence of PONV compared with crystalloid infusion (RR, 0.69; 95% CI, 0.53-0.89). In the subgroup that underwent anesthesia for <3 hours, colloid infusion did not reduce the incidence of PONV compared with crystalloid infusion (RR, 1.32; 95% CI, 0.76-2.27). The requirement for antiemetics was comparable between colloid and crystalloid infusions, with an RR of 0.93 (95% CI, 0.55-1.58).
Colloid administration had a more preventive effect on PONV than crystalloid administration in patients undergoing abdominal surgery under general anesthesia for more than 3 hours but did not show a preventive effect in patients undergoing anesthesia for <3 hours.
充足的静脉补液被推荐作为一种有效的非药物策略,用于减少术后恶心呕吐(PONV),这是全身麻醉最常见且令人困扰的并发症之一。由于既往研究结果不一致,我们旨在评估根据液体类型进行补液对PONV的影响。
我们对随机对照试验(RCT)进行了系统评价和荟萃分析,比较胶体液输注与晶体液输注在全身麻醉术后PONV发生率及术后24小时抢救性使用止吐治疗的必要性方面的差异。同时也研究了根据麻醉持续时间进行液体输注的效果。截至2018年2月,使用MEDLINE、医学文摘数据库、Cochrane对照试验中心注册库、科学引文索引和Scopus进行了文献检索。
我们纳入了8项RCT。与晶体液输注相比,围手术期输注胶体液并未降低PONV发生率,相对危险度为0.87(95%置信区间[CI],0.60 - 1.25)。然而,按麻醉持续时间进行的亚组分析显示出具有统计学意义的亚组效应(P = 0.04,I = 77.4%),这表明根据麻醉持续时间不同,胶体液和晶体液的效果有所差异。在麻醉时间超过3小时的亚组中(这些患者大多接受腹部手术),与晶体液输注相比,胶体液输注显著降低了PONV发生率(RR,0.69;95% CI,0.53 - 0.89)。在麻醉时间<3小时的亚组中,与晶体液输注相比,胶体液输注未降低PONV发生率(RR,1.32;95% CI,0.76 - 2.27)。胶体液和晶体液输注在使用止吐药方面相当,RR为0.93(95% CI,0.55 - 1.58)。
对于全身麻醉下接受腹部手术超过3小时的患者,输注胶体液对PONV的预防作用比输注晶体液更强,但对于麻醉时间<3小时的患者未显示出预防作用。